

Obesity differs from diabetes mellitus in antibody and T-cell responses post-COVID-19 recovery
- PMID: 38642547
- PMCID: PMC11404124
- DOI: 10.1093/cei/uxae030
Obesity differs from diabetes mellitus in antibody and T-cell responses post-COVID-19 recovery
Abstract
Objective: Obesity and type 2 diabetes (DM) are risk factors for severe coronavirus disease 2019 (COVID-19) outcomes, which disproportionately affect South Asian populations. This study aims to investigate the humoral and cellular immune responses to SARS-CoV-2 in adult COVID-19 survivors with overweight/obesity (Ov/Ob, BMI ≥ 23 kg/m2) and DM in Bangladesh.
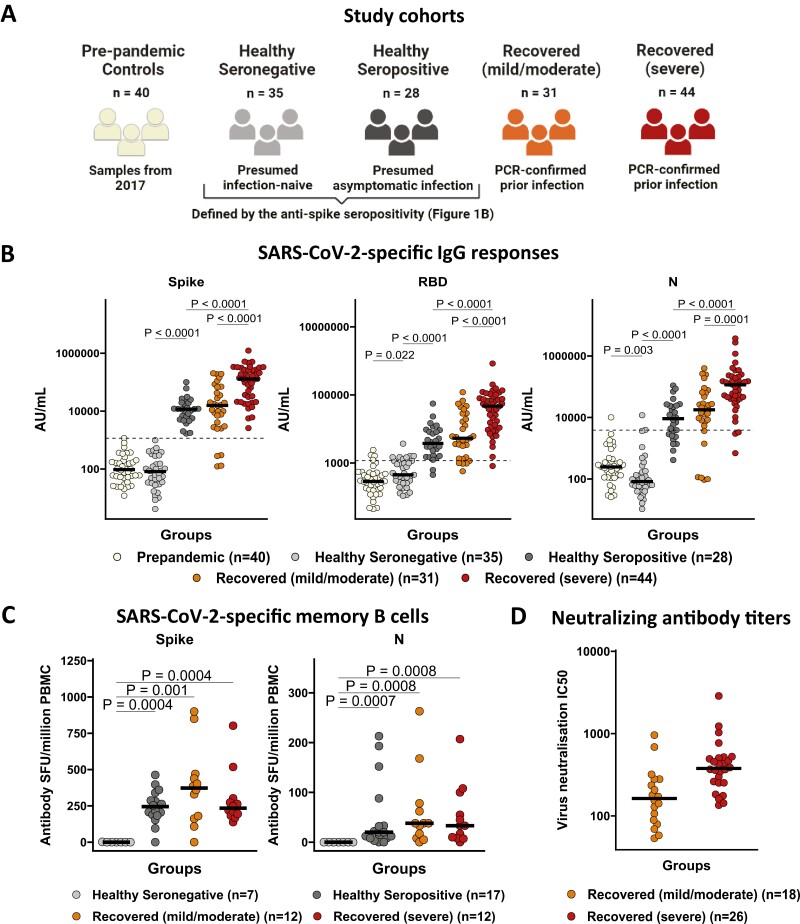
Methods: In this cross-sectional study, SARS-CoV-2-specific antibody and T-cell responses were investigated in 63 healthy and 75 PCR-confirmed COVID-19 recovered individuals in Bangladesh, during the pre-vaccination first wave of the COVID-19 pandemic in 2020.
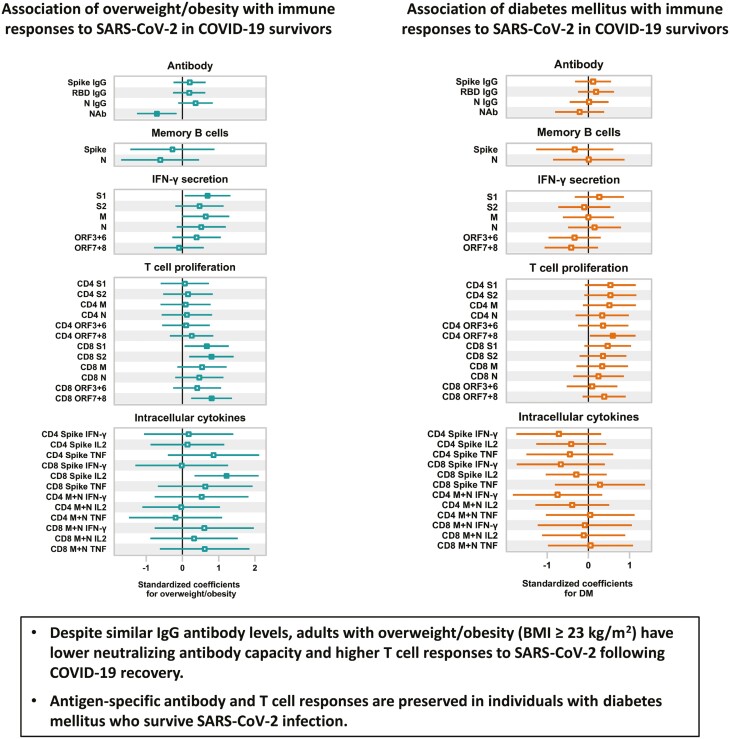
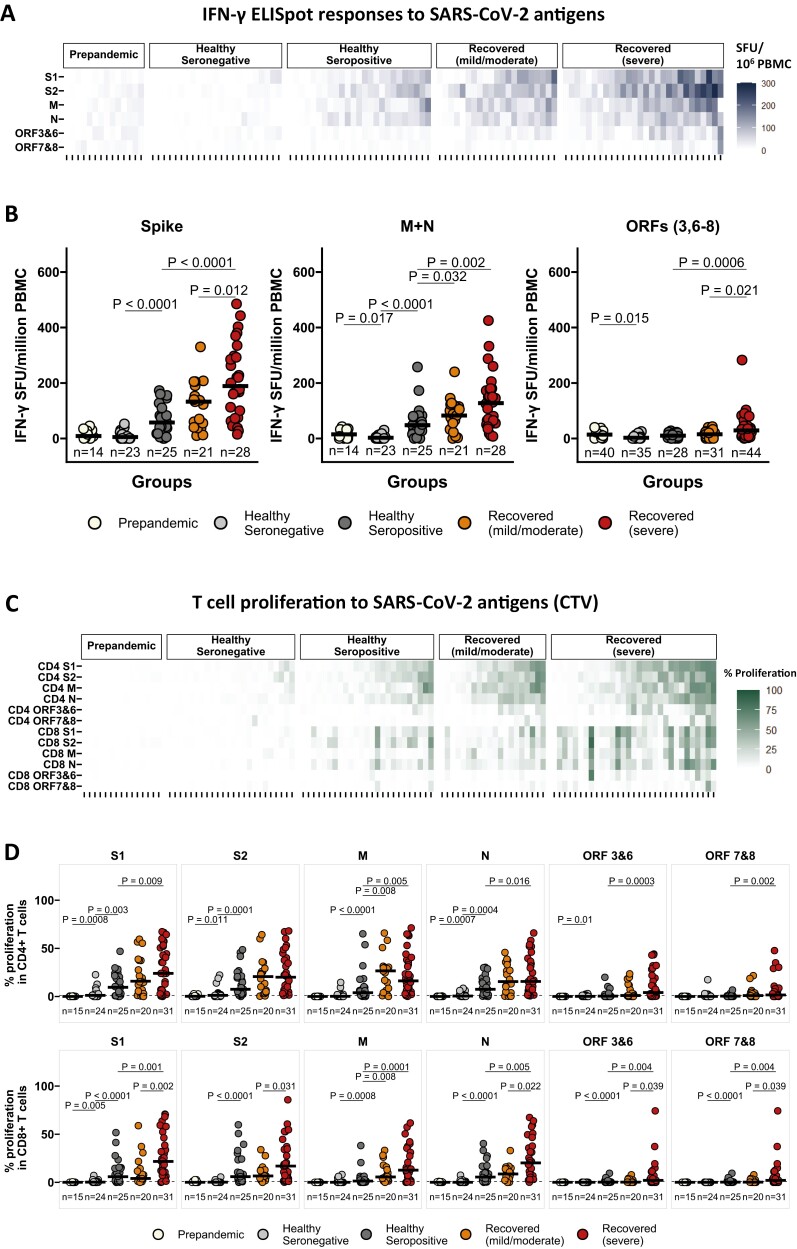
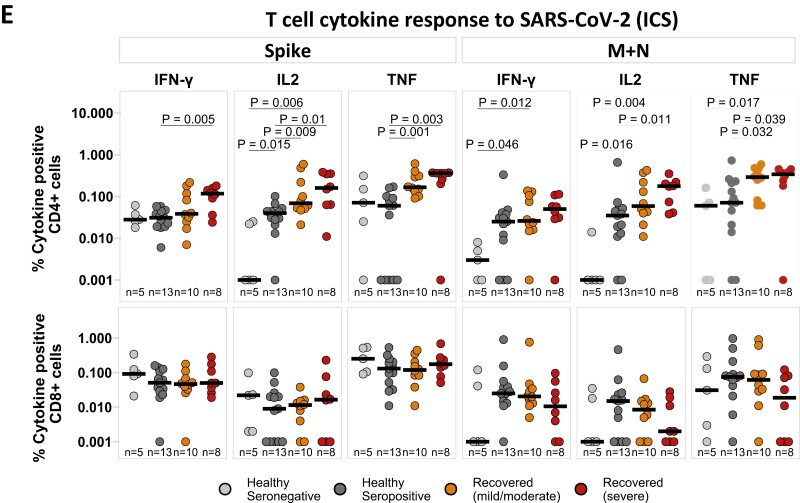
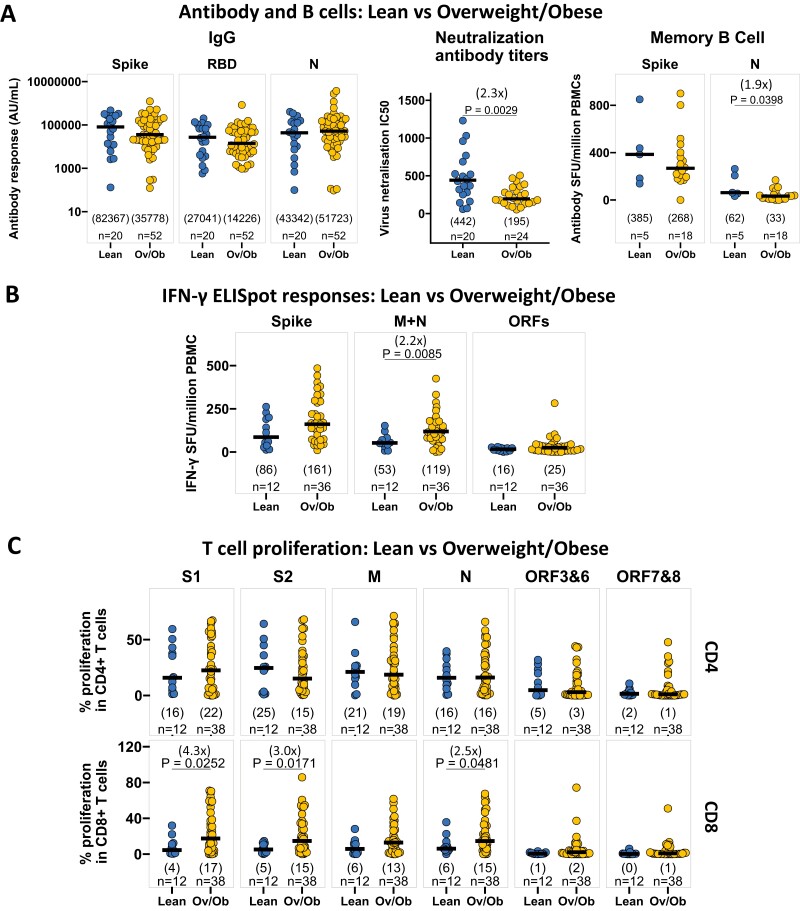
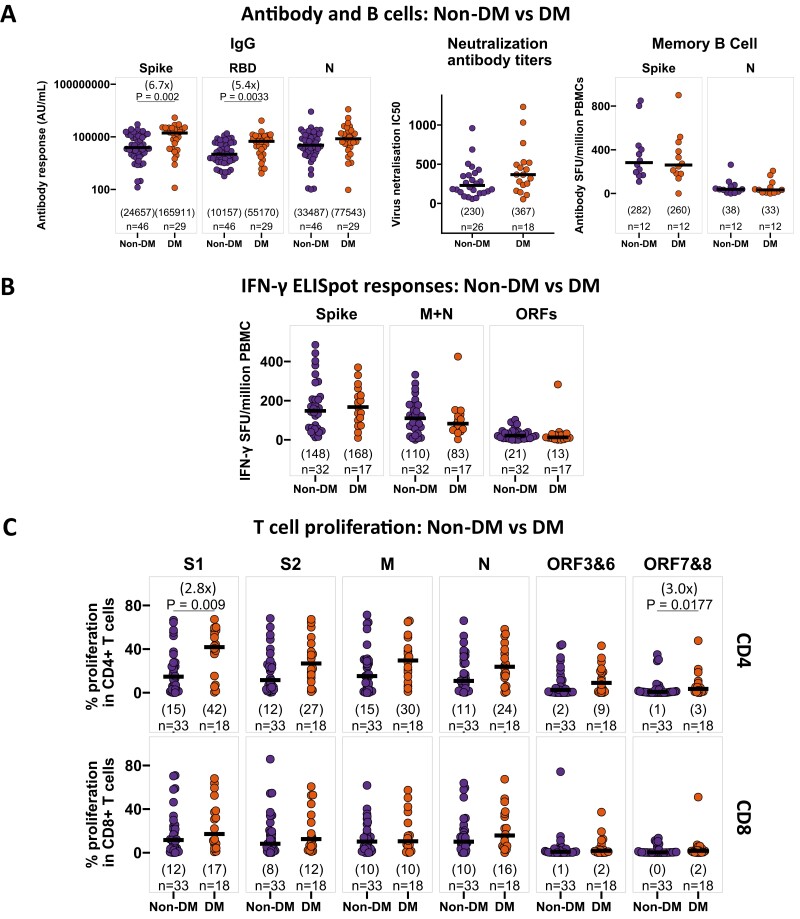
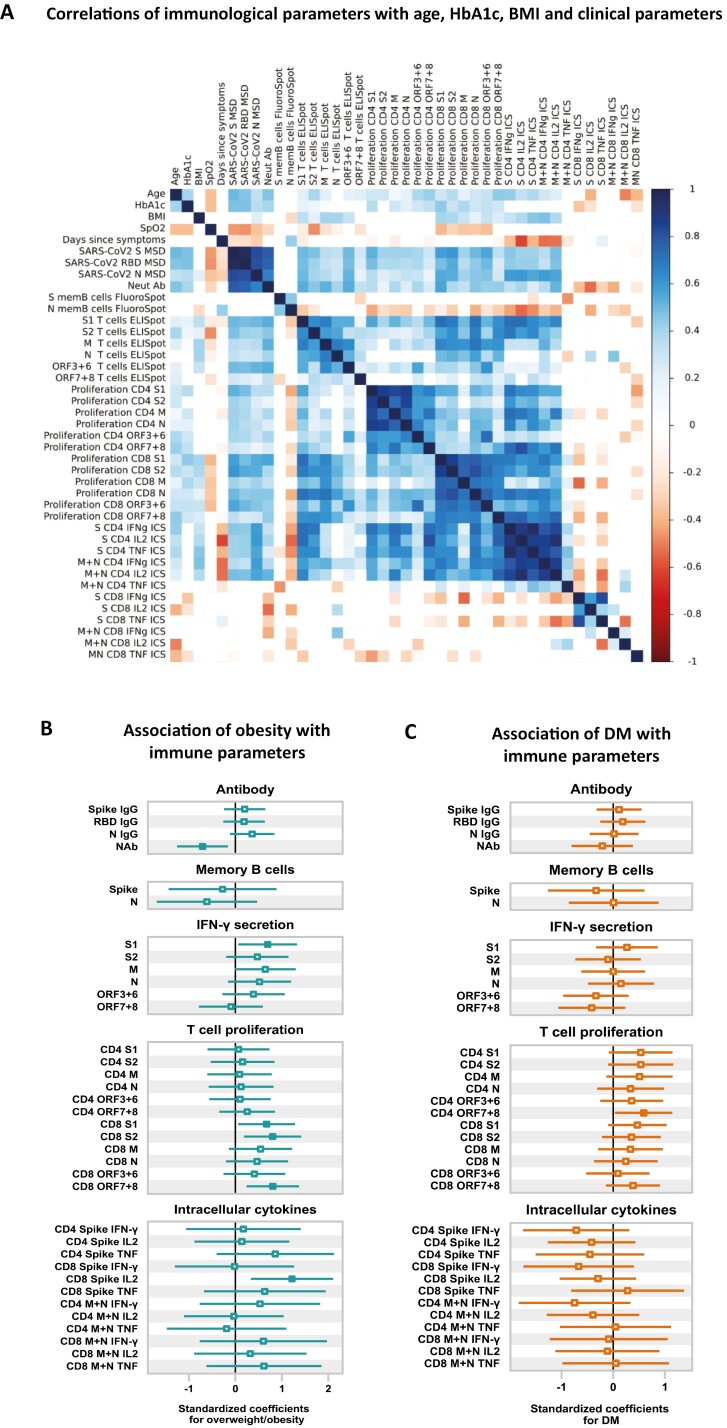
Results: In COVID-19 survivors, SARS-CoV-2 infection induced robust antibody and T-cell responses, which correlated with disease severity. After adjusting for age, sex, DM status, disease severity, and time since onset of symptoms, Ov/Ob was associated with decreased neutralizing antibody titers, and increased SARS-CoV-2 spike-specific IFN-γ response along with increased proliferation and IL-2 production by CD8 + T cells. In contrast, DM was not associated with SARS-CoV-2-specific antibody and T-cell responses after adjustment for obesity and other confounders.
Conclusion: Ov/Ob is associated with lower neutralizing antibody levels and higher T-cell responses to SARS-CoV-2 post-COVID-19 recovery, while antibody or T-cell responses remain unaltered in DM.
Keywords: COVID-19; T cell; antibody; diabetes mellitus; obesity.
© The Author(s) 2024. Published by Oxford University Press on behalf of the British Society for Immunology.
Conflict of interest statement
The authors declared no conflict of interest.
Figures
References
-
- Palaiodimos L, Kokkinidis DG, Li W, Karamanis D, Ognibene J, Arora S, et al. Severe obesity, increasing age and male sex are independently associated with worse in-hospital outcomes, and higher in-hospital mortality, in a cohort of patients with COVID-19 in the Bronx, New York. Metabolism 2020, 108, 154262. doi: 10.1016/j.metabol.2020.154262 - DOI - PMC - PubMed
-
- Hendren NS, De Lemos JA, Ayers C, Das SR, Rao A, Carter S, et al. Association of body mass index and age with morbidity and mortality in patients hospitalized with COVID-19: results from the American Heart Association COVID-19 Cardiovascular Disease Registry. Circulation 2021, 143, 135–44. doi: 10.1161/CIRCULATIONAHA.120.051936 - DOI - PubMed
-
- Gao M, Piernas C, Astbury NM, Hippisley-Cox J, O'Rahilly S, Aveyard P, et al. Associations between body-mass index and COVID-19 severity in 6·9 million people in England: a prospective, community-based, cohort study. The Lancet Diabetes Endocrinol 2021, 9, 350–9. doi: 10.1016/S2213-8587(21)00089-9 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
