

Long-term neuropsychological trajectories in children with epilepsy: does surgery halt decline?
- PMID: 38643018
- PMCID: PMC11292899
- DOI: 10.1093/brain/awae121
Long-term neuropsychological trajectories in children with epilepsy: does surgery halt decline?
Abstract
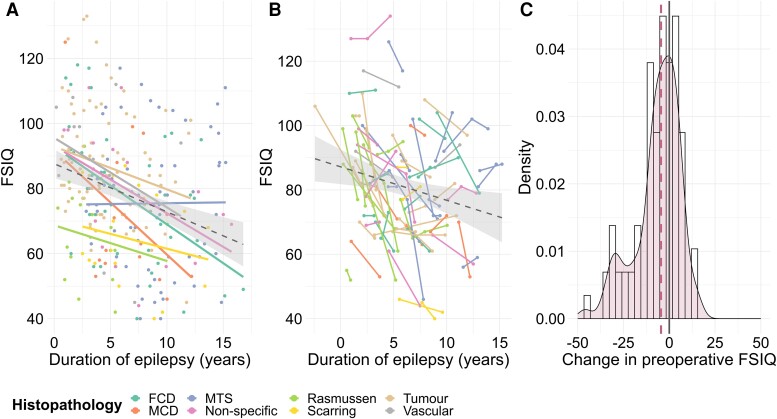
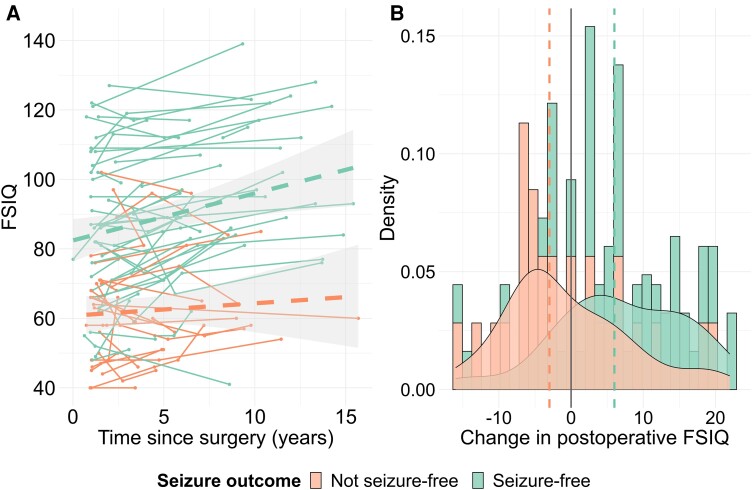
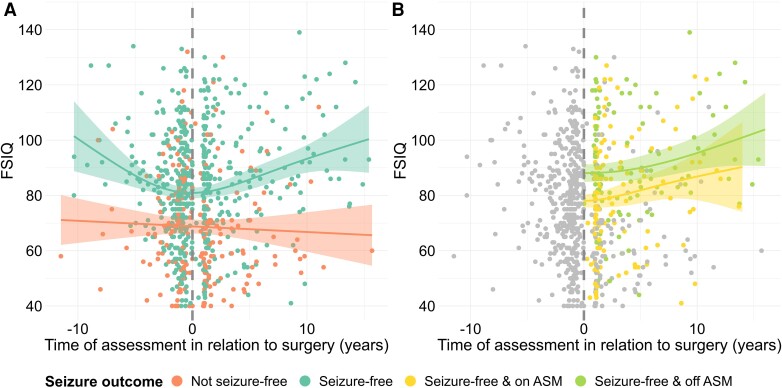
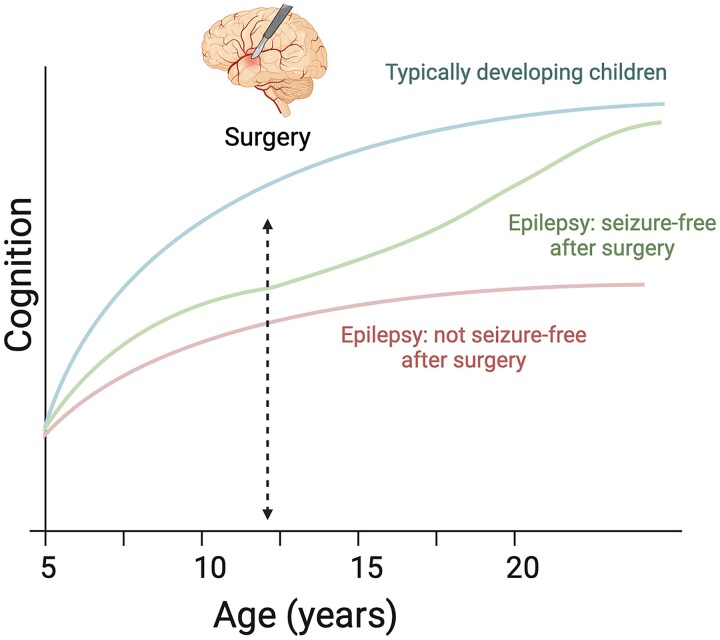
Neuropsychological impairments are common in children with drug-resistant epilepsy. It has been proposed that epilepsy surgery might alleviate these impairments by providing seizure freedom; however, findings from prior studies have been inconsistent. We mapped long-term neuropsychological trajectories in children before and after undergoing epilepsy surgery, to measure the impact of disease course and surgery on functioning. We performed a retrospective cohort study of 882 children who had undergone epilepsy surgery at Great Ormond Street Hospital (1990-2018). We extracted patient information and neuropsychological functioning [obtained from IQ tests (domains: full-scale IQ, verbal IQ, performance IQ, working memory and processing speed) and tests of academic attainment (reading, spelling and numeracy)] and investigated changes in functioning using regression analyses. We identified 500 children (248 females) who had undergone epilepsy surgery [median age at surgery = 11.9 years, interquartile range = (7.8, 15.0)] and neuropsychological assessment. These children showed declines in all domains of neuropsychological functioning in the time leading up to surgery (all P-values ≤0.001; e.g. βFSIQ = -1.9, SEFSIQ = 0.3, PFSIQ < 0.001). Children lost on average one to four points per year, depending on the domain considered; 27%-43% declined by ≥10 points from their first to their last preoperative assessment. At the time of presurgical evaluation, most children (46%-60%) scored one or more standard deviations below the mean (<85) on the different neuropsychological domains; 37% of these met the threshold for intellectual disability (full-scale IQ < 70). On a group level, there was no change in performance from pre- to postoperative assessment on any of the domains (all P-values ≥0.128). However, children who became seizure free through surgery showed higher postoperative neuropsychological performance (e.g. rrb-FSIQ = 0.37, P < 0.001). These children continued to demonstrate improvements in neuropsychological functioning over the course of their long-term follow-up (e.g. βFSIQ = 0.9, SEFSIQ = 0.3, PFSIQ = 0.004). Children who had discontinued antiseizure medication treatment at 1-year follow-up showed an 8- to 13-point advantage in postoperative working memory, processing speed and numeracy, and greater improvements in verbal IQ, working memory, reading and spelling (all P-values ≤0.034) over the postoperative period compared with children who were seizure free and still receiving antiseizure medication. In conclusion, by providing seizure freedom and the opportunity for antiseizure medication cessation, epilepsy surgery might not only halt but reverse the downward trajectory that children with drug-resistant epilepsy display in neuropsychological functioning. To halt this decline as soon as possible or, potentially, to prevent it from occurring in the first place, children with focal epilepsy should be considered for epilepsy surgery as early as possible after diagnosis.
Keywords: IQ; academic attainment; epilepsy surgery; neuropsychology; paediatric; trajectories.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
J.H.C. has acted as an investigator for studies with GW Pharmaceuticals, Zogenix, Vitaflo, Ovid, Marinius, Ultragenyx and Stoke Therapeutics. She has been a speaker and on advisory boards for GW Pharmaceuticals, Zogenix, Biocodex, Stoke Therapeutics, Takeda and Nutricia. All remuneration has been paid to her department. She is president of the International League Against Epilepsy (2021–2025) and chair of the medical boards for Dravet UK, Hope 4 Hypothalamic Hamartoma and Matthew’s friends. M.M.T. has received grants from the Royal Academy of Engineers and LifeArc. He has received honoraria from Medtronic. All remuneration has been paid to his department. L.M. has received personal consultancy fees from Mendelian Ltd, outside the submitted work. A.M. has received honoraria from Biocodex and Nutricia, and provided consultancy to Biogen, outside the submitted work. All other authors report no competing interests.
Figures
Similar articles
-
Academic achievement one year after resective epilepsy surgery in children.Epilepsy Behav. 2015 Jun;47:1-5. doi: 10.1016/j.yebeh.2015.04.062. Epub 2015 May 15. Epilepsy Behav. 2015. PMID: 25988982
-
Long-term cognitive outcome after radiosurgery in epileptic hypothalamic hamartomas and review of the literature.Epilepsia. 2021 Jun;62(6):1369-1381. doi: 10.1111/epi.16896. Epub 2021 Apr 20. Epilepsia. 2021. PMID: 33878213
-
Development of intelligence 4 to 11 years after paediatric epilepsy surgery.J Neuropsychol. 2017 Jun;11(2):161-173. doi: 10.1111/jnp.12081. Epub 2015 Jul 17. J Neuropsychol. 2017. PMID: 26184054
-
Cognitive outcome after epilepsy surgery in children.Brain Dev. 2013 Sep;35(8):721-9. doi: 10.1016/j.braindev.2013.01.011. Epub 2013 Feb 21. Brain Dev. 2013. PMID: 23434294 Review.
-
Evolution of epilepsy comorbidities in seizure free patients: Is no seizure a synonym of no epilepsy?Rev Neurol (Paris). 2025 May;181(5):456-470. doi: 10.1016/j.neurol.2025.04.004. Epub 2025 Apr 16. Rev Neurol (Paris). 2025. PMID: 40246676 Review.
Cited by
-
Longitudinal alterations in brain networks and thalamocortical connectivity in paediatric focal epilepsy: a structural connectomics pilot study.Brain Commun. 2025 Feb 27;7(1):fcaf081. doi: 10.1093/braincomms/fcaf081. eCollection 2025. Brain Commun. 2025. PMID: 40040839 Free PMC article.
-
Cross-sectional and longitudinal changes in category-selectivity in visual cortex following pediatric cortical resection.bioRxiv [Preprint]. 2024 Dec 12:2024.12.08.627367. doi: 10.1101/2024.12.08.627367. bioRxiv. 2024. Update in: Commun Biol. 2025 Aug 12;8(1):1200. doi: 10.1038/s42003-025-08554-2. PMID: 39713452 Free PMC article. Updated. Preprint.
-
Functional resilience of the neural visual recognition system post-pediatric occipitotemporal resection.iScience. 2024 Nov 22;27(12):111440. doi: 10.1016/j.isci.2024.111440. eCollection 2024 Dec 20. iScience. 2024. PMID: 39735436 Free PMC article.
-
Detection of Epileptogenic Focal Cortical Dysplasia Using Graph Neural Networks: A MELD Study.JAMA Neurol. 2025 Feb 24;82(4):397-406. doi: 10.1001/jamaneurol.2024.5406. Online ahead of print. JAMA Neurol. 2025. PMID: 39992650
-
Merritt-Putnam Symposium | Developmental and Epileptic Encephalopathies-Current Concepts and Novel Approaches.Epilepsy Curr. 2025 Mar 25;25(3):229-235. doi: 10.1177/15357597251320142. eCollection 2025 May-Jun. Epilepsy Curr. 2025. PMID: 40161506 Free PMC article. Review.
References
-
- Nickels KC, Zaccariello MJ, Hamiwka LD, Wirrell EC. Cognitive and neurodevelopmental comorbidities in paediatric epilepsy. Nat Rev Neurol. 2016;12:465–476. - PubMed
-
- Camfield CS, Camfield PR. Long-term social outcomes for children with epilepsy. Epilepsia. 2007;48:3–5. - PubMed
-
- Braun KPJ. Preventing cognitive impairment in children with epilepsy. Curr Opin Neurol. 2017;30:140–147. - PubMed
-
- Hermann B, Meador KJ, Gaillard WD, Cramer JA. Cognition across the lifespan: Antiepileptic drugs, epilepsy, or both? Epilepsy Behav. 2010;17:1–5. - PubMed
-
- Cross JH, Reilly C, Gutierrez Delicado E, Smith ML, Malmgren K. Epilepsy surgery for children and adolescents: Evidence-based but underused. Lancet Child Adolesc Health. 2022;6:484–494. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
