

Efficacy of a high-intensity home stretching device and traditional physical therapy in non-operative management of adhesive capsulitis - a prospective, randomized control trial
- PMID: 38643086
- PMCID: PMC11031861
- DOI: 10.1186/s12891-024-07448-4
Efficacy of a high-intensity home stretching device and traditional physical therapy in non-operative management of adhesive capsulitis - a prospective, randomized control trial
Abstract
Background: Historically, in-person physical therapy serves as a foundational component of nonoperative treatment of adhesive capsulitis (AC). This study compares the effectiveness of an at-home high-intensity stretch (HIS) device to traditional physical therapy (PT) and to PT in combination with the HIS device. We hypothesize that the HIS device will be as effective as PT alone or as combination therapy in the first-line treatment of AC and use of the HIS device will exhibit improvement at higher rate.
Methods: Thirty-four patients with idiopathic adhesive capsulitis and a minimum of 12 months follow-up were included in this study. Patients were randomized into one of the three groups: HIS device, PT alone, or HIS device + PT. Passive range of motion (ROM), American Shoulder and Elbow Surgeons (ASES), and Simple Shoulder Test (SST) scores were measured. Additionally, patient satisfaction, compliance and complications were recorded. Paired t-test, ANOVA and Chi-squared tests were used in analysis.
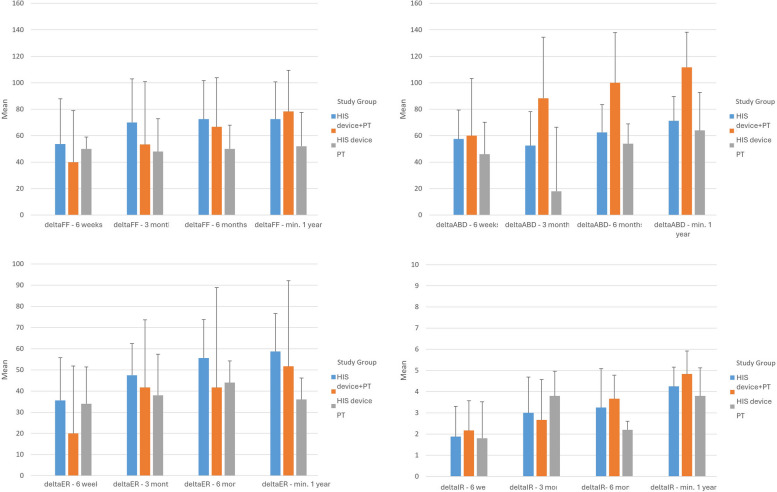
Results: Final ROM in all planes improved for all groups compared to baseline (p < 0.001), with only HIS device group able to restore > 95% of contralateral ROM in all planes at final follow-up. Patients with PT alone were on average slowest to improve ROM from baseline, at 3 months, 6 months, and 1 year in all planes except internal rotation. ASES and SST scores improved for all groups when compared to baseline (p < 0.001). Use of HIS-device resulted in greater improvement in SST and ASES Total scores compared to PT alone (p = 0.045, and p = 0.048, respectively).
Conclusions: Use of an at-home high-intensity stretching device for conservative treatment of idiopathic adhesive capsulitis improves outcomes in ROM and in ASES and SST scores both when used as an adjunct to physical therapy and when used alone.
Trial registration: The study protocol was registered at www.
Clinicaltrials: gov (20/05/2022, NCT05384093).
Keywords: Adhesive capsulitis; High-intensity stretching device; Physical therapy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
