

Days alive and out of hospital for adult female and male cardiac surgery patients: a population-based cohort study
- PMID: 38643088
- PMCID: PMC11031900
- DOI: 10.1186/s12872-024-03862-7
Days alive and out of hospital for adult female and male cardiac surgery patients: a population-based cohort study
Erratum in
-
Correction: Days alive and out of hospital for adult female and male cardiac surgery patients: a population-based cohort study.BMC Cardiovasc Disord. 2024 May 24;24(1):274. doi: 10.1186/s12872-024-03944-6. BMC Cardiovasc Disord. 2024. PMID: 38789938 Free PMC article. No abstract available.
Abstract
Background: Research shows women experience higher mortality than men after cardiac surgery but information on sex-differences during postoperative recovery is limited. Days alive and out of hospital (DAH) combines death, readmission and length of stay, and may better quantify sex-differences during recovery. This main objective is to evaluate (i) how DAH at 30-days varies between sex and surgical procedure, (ii) DAH responsiveness to patient and surgical complexity, and (iii) longer-term prognostic value of DAH.
Methods: We evaluated 111,430 patients (26% female) who underwent one of three types of cardiac surgery (isolated coronary artery bypass [CABG], isolated non-CABG, combination procedures) between 2009 - 2019. Primary outcome was DAH at 30 days (DAH30), secondary outcomes were DAH at 90 days (DAH90) and 180 days (DAH180). Data were stratified by sex and surgical group. Unadjusted and risk-adjusted analyses were conducted to determine the association of DAH with patient-, surgery-, and hospital-level characteristics. Patients were divided into two groups (below and above the 10th percentile) based on the number of days at DAH30. Proportion of patients below the 10th percentile at DAH30 that remained in this group at DAH90 and DAH180 were determined.
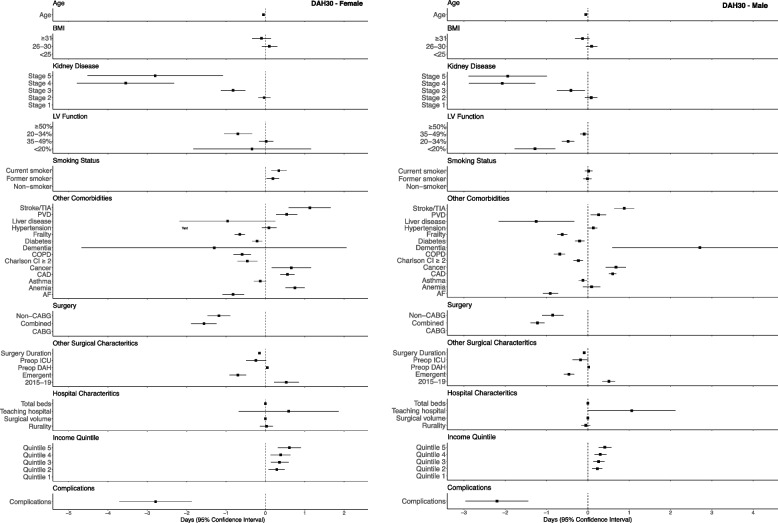
Results: DAH30 were lower for women compared to men (22 vs. 23 days), and seen across all surgical groups (isolated CABG 23 vs. 24, isolated non-CABG 22 vs. 23, combined surgeries 19 vs. 21 days). Clinical risk factors including multimorbidity, socioeconomic status and surgical complexity were associated with lower DAH30 values, but women showed lower values of DAH30 compared to men for many factors. Among patients in the lowest 10th percentile at DAH30, 80% of both females and males remained in the lowest 10th percentile at 90 days, while 72% of females and 76% males remained in that percentile at 180 days.
Conclusion: DAH is a responsive outcome to differences in patient and surgical risk factors. Further research is needed to identify new care pathways to reduce disparities in outcomes between male and female patients.
Keywords: Cardiac surgery; Days at home; Epidemiology; Outcomes; Sex; Validation.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Impact of postoperative intensive care unit utilization on postoperative outcomes in adults undergoing major elective noncardiac surgery.J Clin Anesth. 2020 Jun;62:109707. doi: 10.1016/j.jclinane.2020.109707. Epub 2020 Jan 14. J Clin Anesth. 2020. PMID: 31951918
-
Days alive and out of hospital after fast-track total hip and knee arthroplasty: an observational cohort study in 16 137 patients.Br J Anaesth. 2019 Nov;123(5):671-678. doi: 10.1016/j.bja.2019.07.022. Epub 2019 Aug 29. Br J Anaesth. 2019. PMID: 31474350
-
Hospital costs and factors associated with days alive and at home after surgery (DAH30 ).Med J Aust. 2022 Sep 19;217(6):311-317. doi: 10.5694/mja2.51658. Epub 2022 Jul 18. Med J Aust. 2022. PMID: 35852009 Free PMC article.
-
Stroke Rates Following Surgical Versus Percutaneous Coronary Revascularization.J Am Coll Cardiol. 2018 Jul 24;72(4):386-398. doi: 10.1016/j.jacc.2018.04.071. J Am Coll Cardiol. 2018. PMID: 30025574
-
Does gender influence the likelihood or types of complications following cardiac surgery?Semin Cardiothorac Vasc Anesth. 2004 Dec;8(4):283-95. doi: 10.1177/108925320400800403. Semin Cardiothorac Vasc Anesth. 2004. PMID: 15583790 Review.
Cited by
-
Correction: Days alive and out of hospital for adult female and male cardiac surgery patients: a population-based cohort study.BMC Cardiovasc Disord. 2024 May 24;24(1):274. doi: 10.1186/s12872-024-03944-6. BMC Cardiovasc Disord. 2024. PMID: 38789938 Free PMC article. No abstract available.
References
-
- Saxena A, Dinh D, Smith JA, Shardey G, Reid CM, Newcomb AE. Sex differences in outcomes following isolated coronary artery bypass graft surgery in Australian patients: analysis of the Australasian Society of Cardiac and Thoracic Surgeons cardiac surgery database. Eur J Cardiothorac Surg. 2012;41:755–762. doi: 10.1093/ejcts/ezr039. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
