

Impact of postoperative cerebral complications in acute infective endocarditis: a retrospective single-center study
- PMID: 38643144
- PMCID: PMC11031872
- DOI: 10.1186/s13019-024-02768-x
Impact of postoperative cerebral complications in acute infective endocarditis: a retrospective single-center study
Abstract
Background: The treatment of patients with infective endocarditis (IE) who have preoperative cerebral complications remains less understood. Therefore, this study aimed to retrospectively evaluate the clinical outcomes of patients with acute IE based on preoperative intracranial findings.
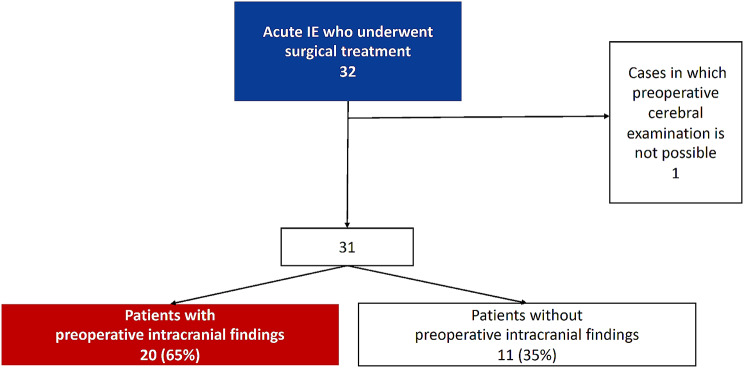
Methods: Of 32 patients with acute IE treated at our hospital between August 2015 and March 2022, 31 patients of whom preoperative intracranial imaging evaluation was available were included in our analysis and compared with those with and without intracranial findings. We controlled the mean arterial blood pressure and activated clotting time (ACT) to prevent abnormally high perfusion pressures and ACTs during cardiopulmonary bypass (CPB). The preoperative background, and postoperative courses focusing on postoperative brain complications were reviewed.
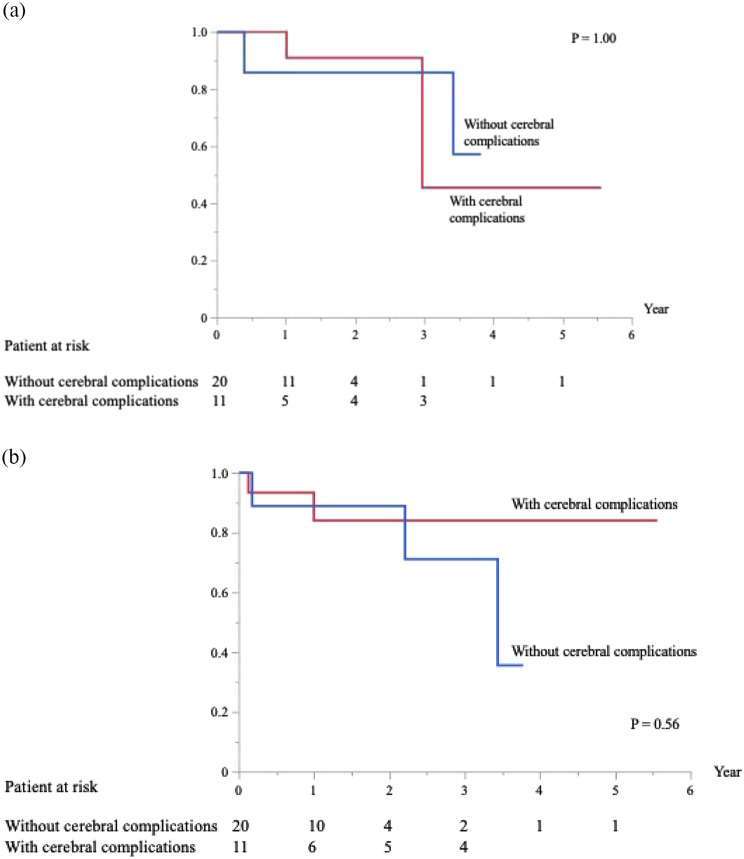
Results: Among the 31 patients, 20 (65%) had preoperative imaging findings. The group with intracranial findings was significantly older, with more embolisms in other organs, positive intraoperative pathology findings, and longer CPB times. A new cerebral hemorrhage developed postoperatively in one patient without intracranial findings. There were no early deaths; two patients had recurrent infections in each group, and one died because of sepsis in the late phase in the group with intracranial findings.
Conclusions: Positive intracranial findings indicated significantly active infectious conditions preoperatively but did not affect the postoperative course. Patients without preoperative cerebral complications can develop serious cerebral hemorrhage. Although meticulous examination of preoperative cerebral complications in all patients with IE is essential, a strategy should be adopted to prevent cerebral hemorrhage, even in patients without intracranial findings.
Keywords: Cerebral hemorrhage; Cerebral infarction; Infective endocarditis; Mycotic aneurysm; Subarachnoid hemorrhage.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Intracranial mycotic aneurysm is associated with cerebral bleeding post-valve surgery for infective endocarditis.Interact Cardiovasc Thorac Surg. 2018 Nov 1;27(5):635-641. doi: 10.1093/icvts/ivy126. Interact Cardiovasc Thorac Surg. 2018. PMID: 29701786
-
Mycotic aneurysm detection rates with cerebral angiography in patients with infective endocarditis.J Neurointerv Surg. 2015 Jun;7(6):449-52. doi: 10.1136/neurintsurg-2014-011124. Epub 2014 Apr 28. J Neurointerv Surg. 2015. PMID: 24778139
-
Can radiological characteristics of preoperative cerebral lesions predict postoperative intracranial haemorrhage in endocarditis patients?Eur J Cardiothorac Surg. 2016 May;49(5):e119-26. doi: 10.1093/ejcts/ezw014. Epub 2016 Feb 16. Eur J Cardiothorac Surg. 2016. PMID: 26888461
-
Neurological complications of infective endocarditis: new breakthroughs in diagnosis and management.Med Mal Infect. 2013 Dec;43(11-12):443-50. doi: 10.1016/j.medmal.2013.09.010. Epub 2013 Nov 9. Med Mal Infect. 2013. PMID: 24215865 Review.
-
What is the optimal timing for surgery in infective endocarditis with cerebrovascular complications?Interact Cardiovasc Thorac Surg. 2012 Jan;14(1):72-80. doi: 10.1093/icvts/ivr010. Epub 2011 Nov 18. Interact Cardiovasc Thorac Surg. 2012. PMID: 22108925 Free PMC article. Review.
References
-
- Lalani T, Cabell CH, Benjamin DK, Lasca O, Naber C, Fowler VG, Jr, et al. Analysis of the impact of early surgery on in-hospital mortality of native valve endocarditis: use of propensity score and instrumental variable methods to adjust for treatment-selection bias. Circulation. 2010;121:1005–13. doi: 10.1161/CIRCULATIONAHA.109.864488. - DOI - PMC - PubMed
-
- García-Cabrera E, Fernández-Hidalgo N, Almirante B, Ivanova-Georgieva R, Noureddine M, Plata A, et al. Neurological complications of infective endocarditis: risk factors, outcome, and impact of cardiac surgery: a multicenter observational study. Circulation. 2013;127:2272–84. doi: 10.1161/CIRCULATIONAHA.112.000813. - DOI - PubMed
-
- Yoshioka D, Toda K, Sakaguchi T, Okazaki S, Yamauchi T, Miyagawa S, et al. Valve surgery in active endocarditis patients complicated by intracranial haemorrhage: the influence of the timing of surgery on neurological. Eur J Cardiothorac Surg. 2014;45:1082–8. doi: 10.1093/ejcts/ezt547. - DOI - PubMed
-
- Baddour LM, Wilson WR, Bayer AS, Fowler VG, Jr, Bolger AF, Levison ME, et al. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the councils on Clinical Cardiology, Stroke, and cardiovascular surgery and anesthesia. Circulation. 2005;111:e394–434. doi: 10.1161/CIRCULATIONAHA.105.165564. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
