

Deviations in RSV epidemiological patterns and population structures in the United States following the COVID-19 pandemic
- PMID: 38643200
- PMCID: PMC11032338
- DOI: 10.1038/s41467-024-47757-9
Deviations in RSV epidemiological patterns and population structures in the United States following the COVID-19 pandemic
Abstract
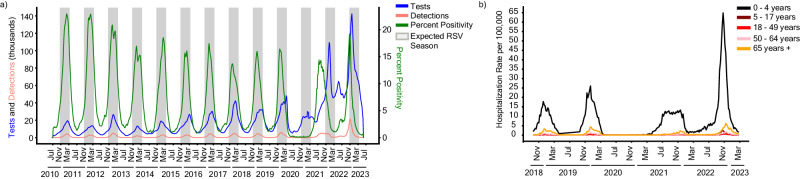
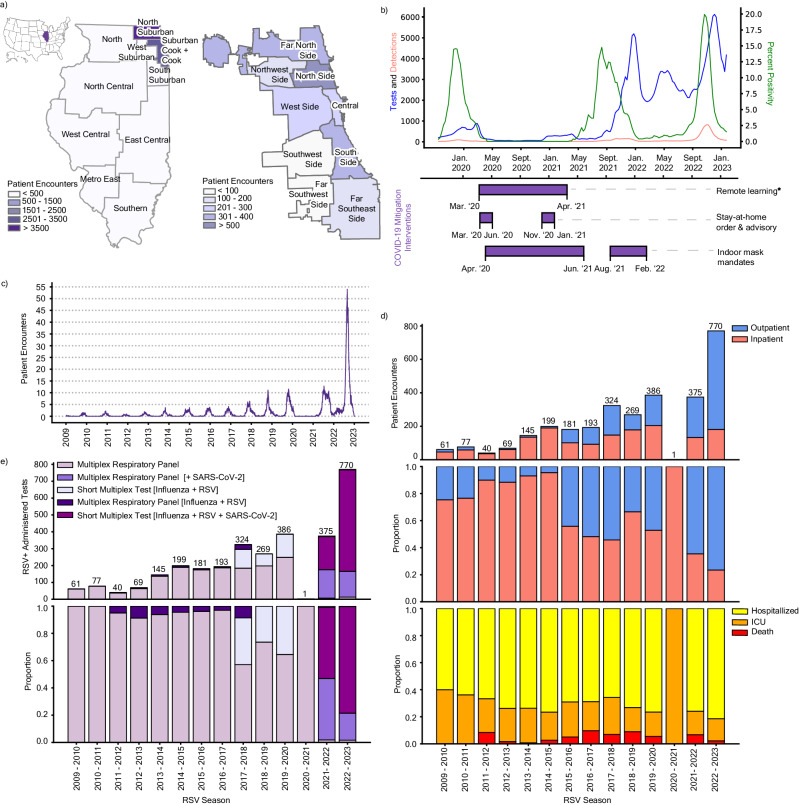
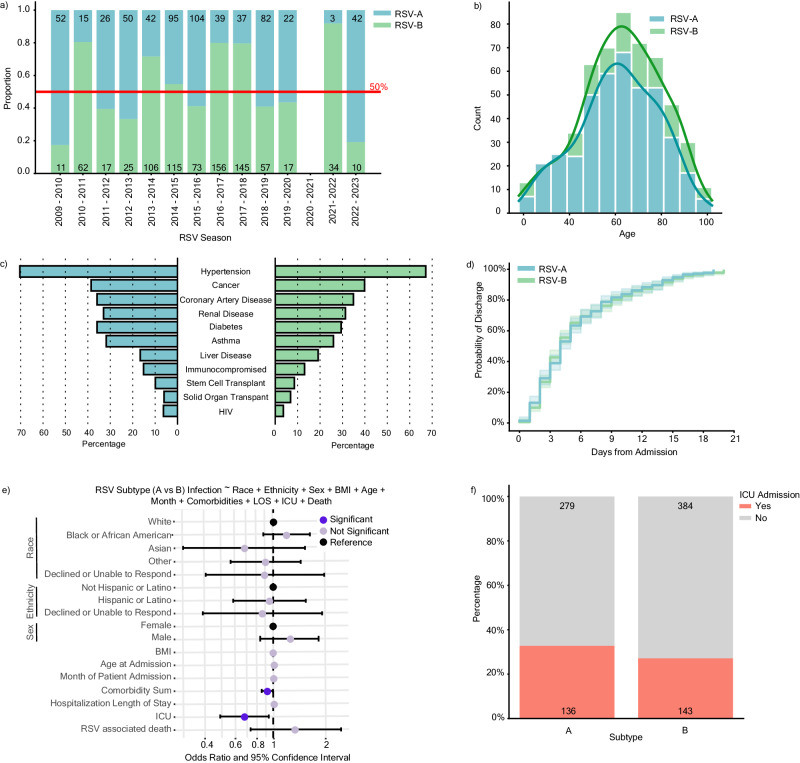
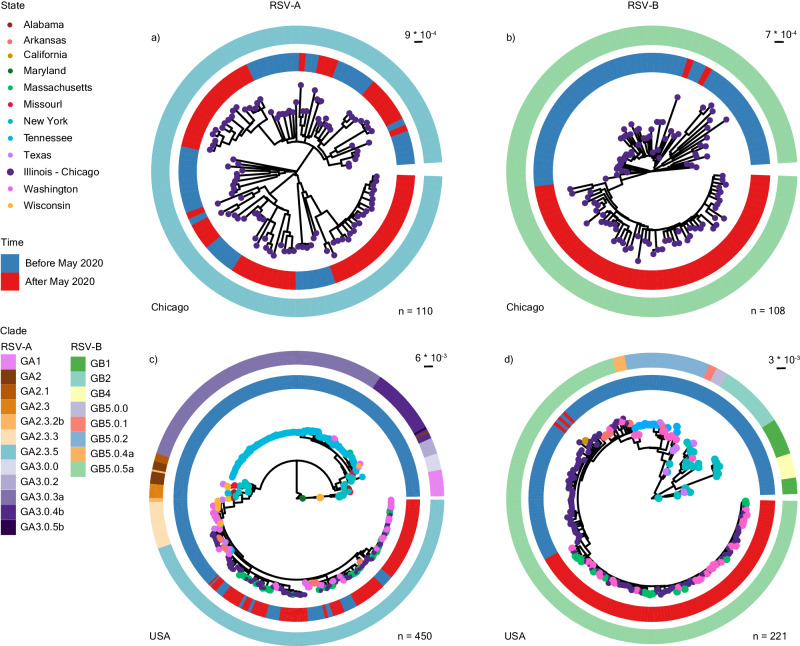
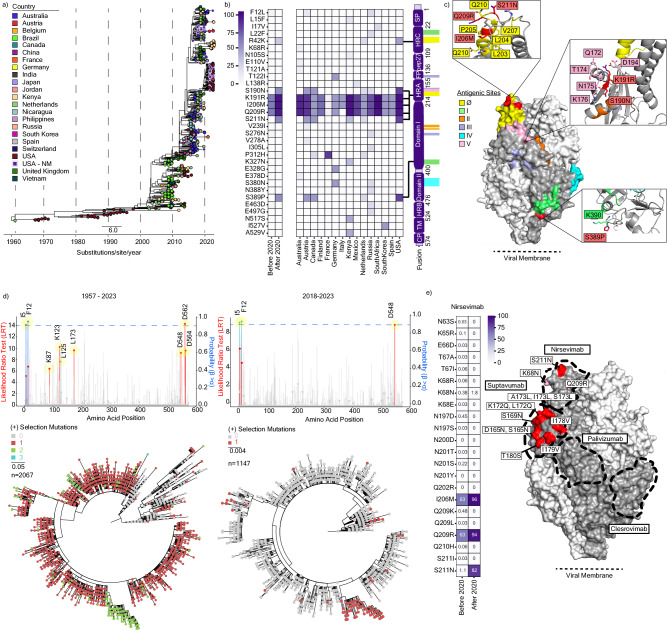
Respiratory Syncytial Virus (RSV) is a leading cause of acute respiratory tract infection, with the greatest impact on infants, immunocompromised individuals, and older adults. RSV prevalence decreased substantially in the United States (US) following the implementation of COVID-19-related non-pharmaceutical interventions but later rebounded with abnormal seasonality. The biological and epidemiological factors underlying this altered behavior remain poorly defined. In this retrospective cohort study from 2009 to 2023 in Chicago, Illinois, US, we examined RSV epidemiology, clinical severity, and genetic diversity. We found that changes in RSV diagnostic platforms drove increased detections in outpatient settings post-2020 and that hospitalized adults infected with RSV-A were at higher risk of intensive care admission than those with RSV-B. While population structures of RSV-A remained unchanged, RSV-B exhibited a genetic shift into geographically distinct clusters. Mutations in the antigenic regions of the fusion protein suggest convergent evolution with potential implications for vaccine and therapeutic development.
© 2024. The Author(s).
Conflict of interest statement
M.G.I. declares that research support from GSK was paid to his previous institution, Northwestern University; he received consulting fees from Adagio Therapeutics, ADMA Biologics, Adamis Pharmaceuticals, AlloVir, Atea, Cidara Therapeutics, Genentech/Roche, Janssen, Shionogi, Takeda, Talaris, and Eurofins Viracor; and payment for participating in data safety monitoring boards or advisory boards from Adamis Pharmaceuticals, AlloVir, National Institutes of Health, CSL Behring, Janssen, Merck, Seqirus, Takeda, and Talaris; all of these ended in December 2022; M.G.I. also receives author royalties from UpToDate, which is ongoing. J.F.H. received research support, paid to Northwestern University, from Gilead Sciences and is a paid consultant for Merck. E.R.G has previously been a paid consultant for Merck. All other authors declare no conflicts of interest.
Figures
Update of
-
Altered RSV Epidemiology and Genetic Diversity Following the COVID-19 Pandemic.Res Sq [Preprint]. 2023 Dec 15:rs.3.rs-3712859. doi: 10.21203/rs.3.rs-3712859/v1. Res Sq. 2023. Update in: Nat Commun. 2024 Apr 20;15(1):3374. doi: 10.1038/s41467-024-47757-9. PMID: 38168164 Free PMC article. Updated. Preprint.
References
-
- Jo KJ, Hwang YH, Kyung Y, Lee J-S, Park SE. 2631. The impact of the COVID-19 pandemic on seasonal respiratory virus circulation in Korean children. Open Forum Infect. Dis. 2023;10:ofad500.2243.
-
- IDWR Comparison graph with the past 10 years (weekly report) -RSV Infection -. https://www.niid.go.jp/niid/en/10/2096-weeklygraph/1661-21rsv.html.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
