

Non-invasive biomarkers for spontaneous intracranial hypotension (SIH) through phase-contrast MRI
- PMID: 38643444
- PMCID: PMC11233306
- DOI: 10.1007/s00415-024-12365-6
Non-invasive biomarkers for spontaneous intracranial hypotension (SIH) through phase-contrast MRI
Abstract
Background and objective: Spontaneous intracranial hypotension (SIH) is an underdiagnosed disease. To depict the accurate diagnosis can be demanding; especially the detection of CSF-venous fistulas poses many challenges. Potential dynamic biomarkers have been identified through non-invasive phase-contrast MRI in a limited subset of SIH patients with evidence of spinal longitudinal extradural collection. This study aimed to explore these biomarkers related to spinal cord motion and CSF velocities in a broader SIH cohort.
Methods: A retrospective, monocentric pooled-data analysis was conducted of patients suspected to suffer from SIH who underwent phase-contrast MRI for spinal cord and CSF velocity measurements at segment C2/C3 referred to a tertiary center between February 2022 and June 2023. Velocity ranges (mm/s), total displacement (mm), and further derivatives were assessed and compared to data from the database of 70 healthy controls.
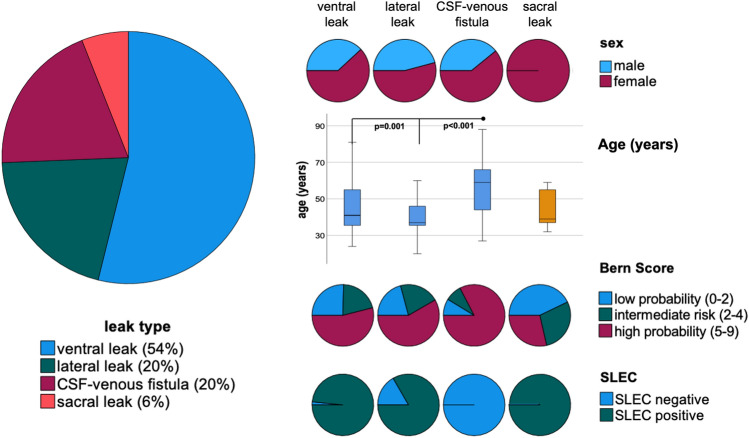
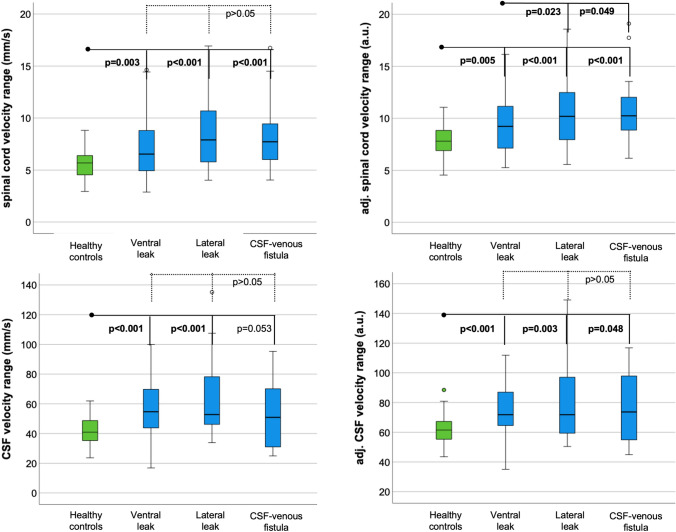
Results: In 117 patients, a leak was located (54% ventral leak, 20% lateral leak, 20% CSF-venous fistulas, 6% sacral leaks). SIH patients showed larger spinal cord and CSF velocities than healthy controls: e.g., velocity range 7.6 ± 3 mm/s vs. 5.6 ± 1.4 mm/s, 56 ± 21 mm/s vs. 42 ± 10 mm/s, p < 0.001, respectively. Patients with lateral leaks and CSF-venous fistulas exhibited an exceptionally heightened level of spinal cord motion (e.g., velocity range 8.4 ± 3.3 mm/s; 8.2 ± 3.1 mm/s vs. 5.6 ± 1.4 mm/s, p < 0.001, respectively).
Conclusion: Phase-contrast MRI might become a valuable tool for SIH diagnosis, especially in patients with CSF-venous fistulas without evidence of spinal extradural fluid collection.
Keywords: CSF flow; CSF–venous fistula; Phase-contrast MRI; Spinal cord motion; Spontaneous intracranial hypotension.
© 2024. The Author(s).
Conflict of interest statement
H. Urbach: honoraria for lectures from Biogen, Eisai, Mbits, Lilly, Co-Editor Clin Neuroradiol. All other authors report no conflict of interest.
Figures


References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
