

Associations between static and dynamic changes of platelet counts and in-hospital mortality in critical patients with acute heart failure
- PMID: 38644461
- PMCID: PMC11033279
- DOI: 10.1038/s41598-024-59892-w
Associations between static and dynamic changes of platelet counts and in-hospital mortality in critical patients with acute heart failure
Abstract
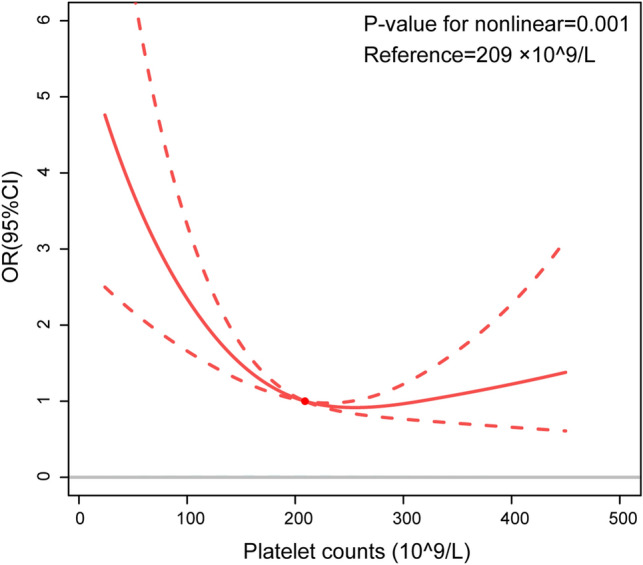
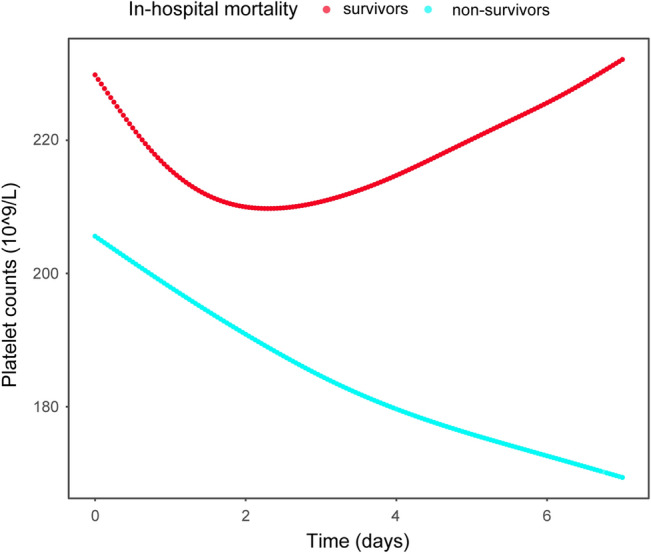
To investigate the predictive value of baseline platelet count and its short-term dynamic changes in the prognosis of patients with acute heart failure (AHF) in the intensive care unit. Patients diagnosed with AHF in the medical information mart for intensive care III and their clinical data were retrospectively filtered. Patients were divided into survivor and non-survivor groups based on their prognosis during hospitalization, and differences in baseline data between groups were compared. Logistic regression models and restricted cubic spline (RCS) plots were performed to evaluate the relationship between baseline platelet counts and in-hospital mortality. Changes and trends in platelet counts were compared between the survivor and non-survivor groups after adjusting for confounders with the generalized additive mixing model (GAMM). A total of 2930 critical patients with acute heart failure were included, of which 2720 were survivors and 210 were non-survivors. Multiple logistic regression models revealed that baseline platelet count was an independent factor in hospital mortality (OR 0.997, 95% CI 0.994-0.999, P-value = 0.018). The RCS plot demonstrated a U-shaped dose-response relationship between baseline platelet count and in-hospital mortality. GAMM analysis suggested that the platelet counts decreased and then increased in the survivor group and gradually decreased in the non-survivor group, with a gradual increase of difference between two groups. After adjusting for confounders, the mean daily increase was -6.014 (95% CI -7.076-4.953, P-value < 0.001). Baseline platelet demonstrated a U-shaped dose-response relationship with adverse outcomes in critical patients with AHF. Early elevation of platelet was correlated with higher in-hospital mortality, indicating that tracking early changes in platelet might help determine the short-term prognosis of critical patients with AHF.
Keywords: Acute heart failure; Change; Generalized additive mixed model; In-hospital mortality; Platelet count.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
- JSKJ-KTQN-2022-11/The Shanghai Jinshan District Health Commission Project Fund
- JSKJ-KTMS-2020-09/The Shanghai Jinshan District Health Commission Project Fund
- 3-25-00SSF-22/Shanghai University of Medical & Health Sciences Research Fund Project
- 2022-WS-61/Shanghai Jinshan District Medical and Health Science and Technology Innovation Fund Project
LinkOut - more resources
Full Text Sources
Medical
