

This is a preprint.
Network localization of pediatric lesion-induced dystonia
- PMID: 38645071
- PMCID: PMC11030491
- DOI: 10.1101/2024.04.06.24305421
Network localization of pediatric lesion-induced dystonia
Update in
-
Network Localization of Pediatric Lesion-Induced Dystonia.Ann Neurol. 2025 Jul;98(1):152-162. doi: 10.1002/ana.27224. Epub 2025 Mar 10. Ann Neurol. 2025. PMID: 40059836
Abstract
Objective: Dystonia is a movement disorder defined by involuntary muscle contractions leading to abnormal postures or twisting and repetitive movements. Classically dystonia has been thought of as a disorder of the basal ganglia, but newer results in idiopathic dystonia and lesion-induced dystonia in adults point to broader motor network dysfunction spanning the basal ganglia, cerebellum, premotor cortex, sensorimotor, and frontoparietal regions. It is unclear whether a similar network is shared between different etiologies of pediatric lesion-induced dystonia.
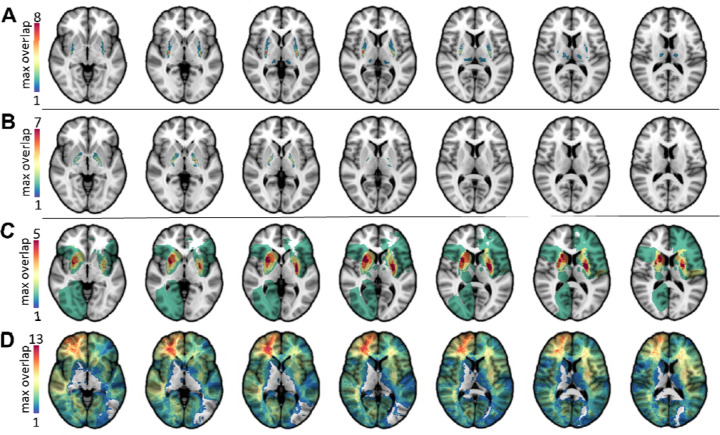
Methods: Three cohorts of pediatric patients with lesion-induced dystonia were identified. The lesion etiologies included hypoxia, kernicterus, and stroke versus comparison subjects with acquired lesions not associated with dystonia. Multivariate lesion-symptom mapping and lesion network mapping were used to evaluate the anatomy and networks associated with dystonia.
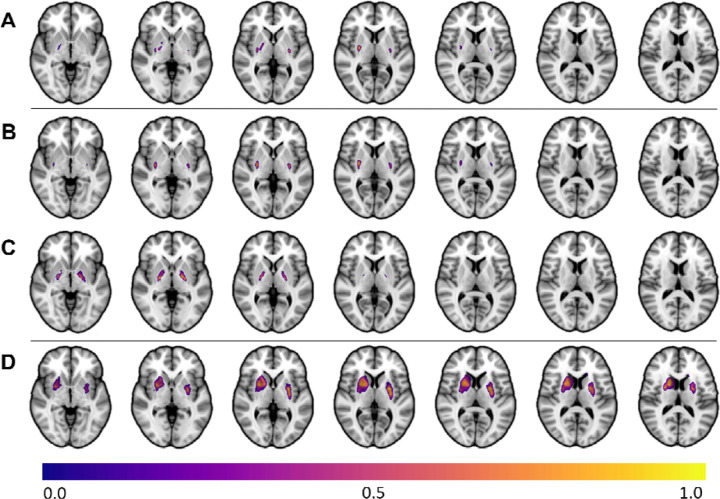
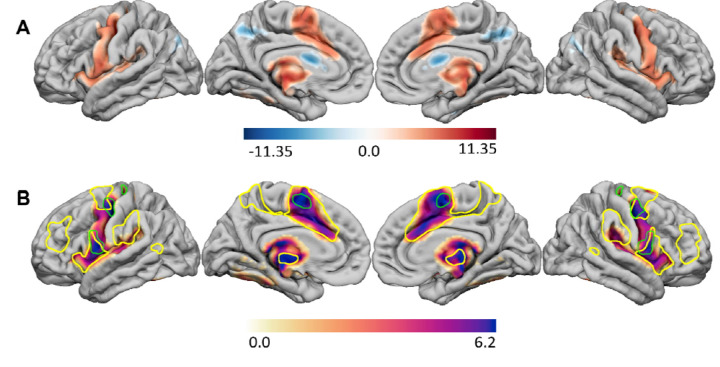
Results: Multivariate lesion-symptom mapping showed that lesions of the putamen (stroke: r = 0.50, p <0.01; hypoxia, r = 0.64, p <0.001) and globus pallidus (kernicterus, r = 0.61, p <0.01) were associated with dystonia. Lesion network mapping using normative connectome data from healthy children demonstrated that these regional findings occurred within a common brain-wide network that involves the basal ganglia, anterior and medial cerebellum, and cortical regions that overlap the cingulo-opercular and somato-cognitive-action networks.
Interpretation: We interpret these findings as novel evidence for a unified dystonia brain network that involves the somato-cognitive-action network, which is involved in higher order coordination of movement. Elucidation of this network gives insight into the functional origins of dystonia and provides novel targets to investigate for therapeutic intervention.
Conflict of interest statement
Conflicts of Interest: No authors have any conflicts of interest to report.
Figures
Similar articles
-
Network Localization of Pediatric Lesion-Induced Dystonia.Ann Neurol. 2025 Jul;98(1):152-162. doi: 10.1002/ana.27224. Epub 2025 Mar 10. Ann Neurol. 2025. PMID: 40059836
-
Network localization of cervical dystonia based on causal brain lesions.Brain. 2019 Jun 1;142(6):1660-1674. doi: 10.1093/brain/awz112. Brain. 2019. PMID: 31099831 Free PMC article.
-
Somato-cognitive action network in laryngeal and focal hand dystonia sensorimotor dysfunction.medRxiv [Preprint]. 2025 Mar 7:2025.02.21.25322612. doi: 10.1101/2025.02.21.25322612. medRxiv. 2025. PMID: 40093209 Free PMC article. Preprint.
-
Contribution of TMS and rTMS in the Understanding of the Pathophysiology and in the Treatment of Dystonia.Front Neural Circuits. 2016 Nov 10;10:90. doi: 10.3389/fncir.2016.00090. eCollection 2016. Front Neural Circuits. 2016. PMID: 27891079 Free PMC article. Review.
-
The neurobiological basis for novel experimental therapeutics in dystonia.Neurobiol Dis. 2019 Oct;130:104526. doi: 10.1016/j.nbd.2019.104526. Epub 2019 Jul 4. Neurobiol Dis. 2019. PMID: 31279827 Free PMC article. Review.
References
-
- Fehlings D, Brown L, Harvey A, Himmelmann K, Lin JP, Macintosh A, Mink JW, Monbaliu E, Rice J, Silver J, Switzer L, Walters I. Bottom Line ‘Evidence-Informed’ Recommendations for the Management of Dystonia in Individuals with Cerebral Palsy: American Academy for Cerebral Palsy and Developmental Medicine Care Pathways; 2016. [April 20, 2023]. Available from: https://www.aacpdm.org/publications/care-pathways/dystonia-in-cerebral-p....
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources