

Individualized positive end-expiratory pressure reduces driving pressure in obese patients during laparoscopic surgery under pneumoperitoneum: a randomized clinical trial
- PMID: 38645690
- PMCID: PMC11026699
- DOI: 10.3389/fphys.2024.1383167
Individualized positive end-expiratory pressure reduces driving pressure in obese patients during laparoscopic surgery under pneumoperitoneum: a randomized clinical trial
Abstract
Introduction: During pneumoperitoneum (PNP), airway driving pressure (ΔPRS) increases due to the stiffness of the chest wall and cephalic shift of the diaphragm, which favors atelectasis. In addition, depending on the mechanical power (MP) formulas, they may lead to different interpretations.
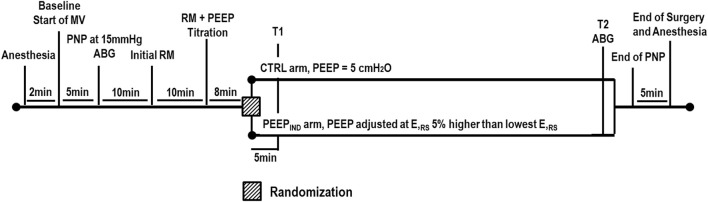
Methods: Patients >18 years of age with body mass index >35 kg/m2 were included in a single-center randomized controlled trial during their admission for bariatric surgery by abdominal laparoscopy. Intra-abdominal pressure was set at 15 mmHg at the pneumoperitoneum time point (PNP). After the recruitment maneuver, the lowest respiratory system elastance (ERS) was detected during the positive end-expiratory pressure (PEEP) step-wise decrement. Patients were randomized to the 1) CTRL group: ventilated with PEEP of 5 cmH2O and 2) PEEPIND group: ventilated with PEEP value associated with ERS that is 5% higher than its lowest level. Respiratory system mechanics and mean arterial pressure (MAP) were assessed at the PNP, 5 min after randomization (T1), and at the end of the ventilation protocol (T2); arterial blood gas was assessed at PNP and T2. ΔPRS was the primary outcome. Three MP formulas were used: MPA, which computes static PEEP × volume, elastic, and resistive components; MPB, which computes only the elastic component; and MPC, which computes static PEEP × volume, elastic, and resistive components without inspiratory holds.
Results: Twenty-eight patients were assessed for eligibility: eight were not included and 20 patients were randomized and allocated to CTRL and PEEPIND groups (n = 10/group). The PEEPIND ventilator strategy reduced ΔPRS when compared with the CTRL group (PEEPIND, 13 ± 2 cmH2O; CTRL, 22 ± 4 cmH2O; p < 0.001). Oxygenation improved in the PEEPIND group when compared with the CTRL group (p = 0.029), whereas MAP was comparable between the PEEPIND and CTRL groups. At the end of surgery, MPA and MPB were correlated in both the CTRL (rho = 0.71, p = 0.019) and PEEPIND (rho = 0.84, p = 0.020) groups but showed different bias (CTRL, -1.9 J/min; PEEPIND, +10.0 J/min). At the end of the surgery, MPA and MPC were correlated in both the CTRL (rho = 0.71, p = 0.019) and PEEPIND (rho = 0.84, p = 0.020) groups but showed different bias (CTRL, -1.9 J/min; PEEPIND, +10.0 J/min).
Conclusion: Individualized PEEP was associated with a reduction in ΔPRS and an improvement in oxygenation with comparable MAP. The MP, which solely computes the elastic component, better reflected the improvement in ΔPRS observed in the individualized PEEP group.
Clinical trial registration: The protocol was registered at the Brazilian Registry of Clinical Trials (U1111-1220-7296).
Keywords: laparoscopy; obesity; positive end-expiratory; pressure; respiratory mechanics.
Copyright © 2024 Xavier, Coelho, Ferreira, Cota y Raposeiras, Duran, Silva, Motta-Ribeiro, Camilo, Carvalho and Silva.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures





References
-
- Bluth T., Serpa Neto A., Schultz M. J., Pelosi P., Gama de Abreu M., Wrigge H., et al. (2019). Effect of intraoperative high positive end-expiratory pressure (PEEP) with recruitment maneuvers vs low PEEP on postoperative pulmonary complications in obese patients: a randomized clinical trial. JAMA 321, 2292–2305. 10.1001/jama.2019.7505 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous