

High lipoprotein(a): Actionable strategies for risk assessment and mitigation
- PMID: 38646021
- PMCID: PMC11031736
- DOI: 10.1016/j.ajpc.2024.100651
High lipoprotein(a): Actionable strategies for risk assessment and mitigation
Abstract
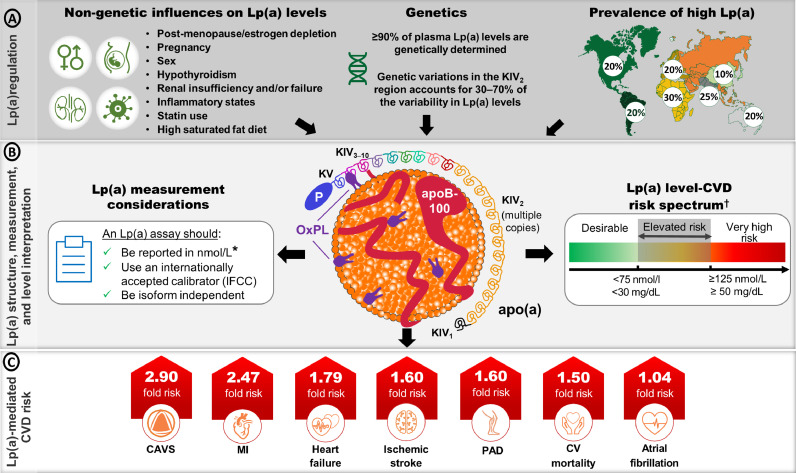
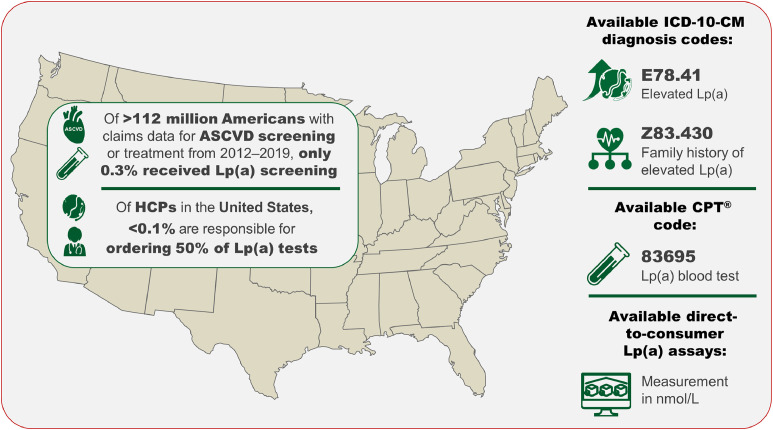
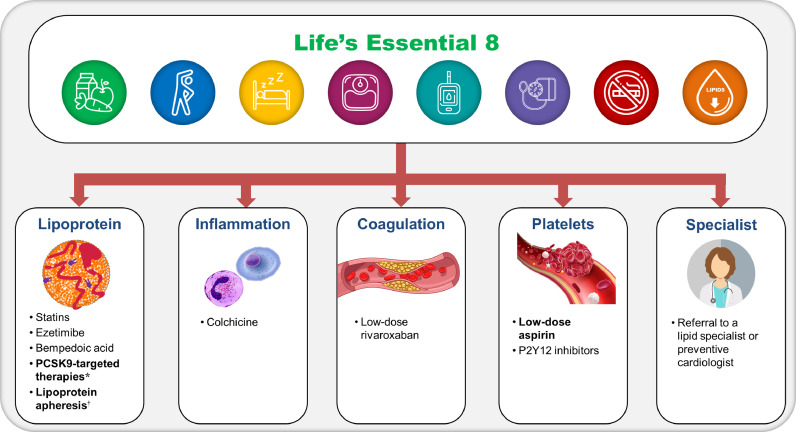
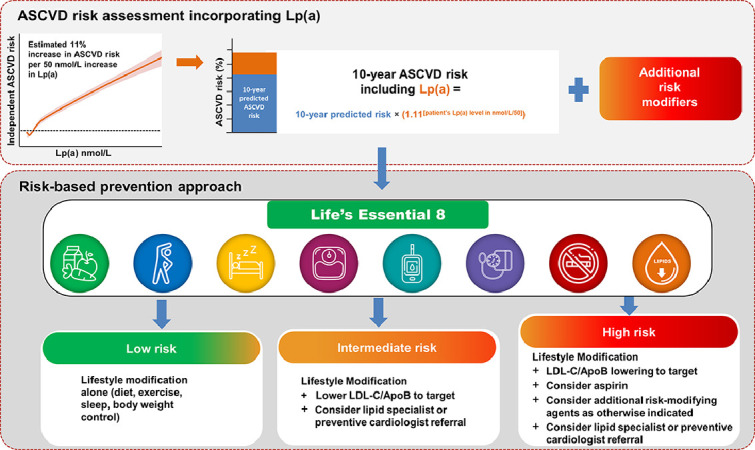
High levels of lipoprotein(a) [Lp(a)] are causal for atherosclerotic cardiovascular disease (ASCVD). Lp(a) is the most prevalent inherited dyslipidemia and strongest genetic ASCVD risk factor. This risk persists in the presence of at target, guideline-recommended, LDL-C levels and adherence to lifestyle modifications. Epidemiological and genetic evidence supporting its causal role in ASCVD and calcific aortic stenosis continues to accumulate, although various facets regarding Lp(a) biology (genetics, pathophysiology, and expression across race/ethnic groups) are not yet fully understood. The evolving nature of clinical guidelines and consensus statements recommending universal measurements of Lp(a) and the scientific data supporting its role in multiple disease states reinforce the clinical merit to start population screening for Lp(a) now. There is a current gap in the implementation of recommendations for primary and secondary cardiovascular disease (CVD) prevention in those with high Lp(a), in part due to a lack of protocols for management strategies. Importantly, targeted apolipoprotein(a) [apo(a)]-lowering therapies that reduce Lp(a) levels in patients with high Lp(a) are in phase 3 clinical development. This review focuses on the identification and clinical management of patients with high Lp(a). Specifically, we highlight the clinical value of measuring Lp(a) and its use in determining Lp(a)-associated CVD risk by providing actionable guidance, based on scientific knowledge, that can be utilized now to mitigate risk caused by high Lp(a).
Keywords: Cardiovascular Disease (CVD); Lipoprotein(a) [Lp(a)]; Lp(a) testing; Risk mitigation.
© 2024 The Authors. Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
-
- Berg K. A new serum type system in man–the Lp system. Acta Pathol Microbiol Scand. 1963;59:369–382. - PubMed
-
- Nestel P., Loh W.J., Ward N.C., Watts G.F. New horizons: revival of lipoprotein (a) as a risk factor for cardiovascular disease. J Clin Endocrinol Metab. 2022;107:e4281–e4294. - PubMed
-
- Wilson D.P., Jacobson T.A., Jones P.H., et al. Use of lipoprotein(a) in clinical practice: a biomarker whose time has come. A scientific statement from the National Lipid Association. J Clin Lipidol. 2019;13:374–392. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
