

Lipoprotein(a): Emerging insights and therapeutics
- PMID: 38646022
- PMCID: PMC11033089
- DOI: 10.1016/j.ajpc.2024.100641
Lipoprotein(a): Emerging insights and therapeutics
Abstract
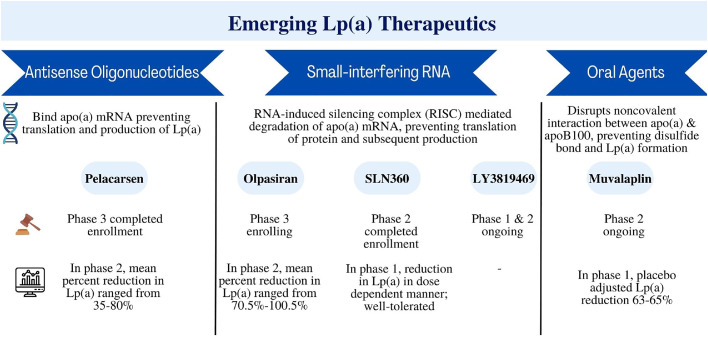
The strong association between lipoprotein (a) [Lp(a)] and atherosclerotic cardiovascular disease has led to considerations of Lp(a) being a potential target for mitigating residual cardiovascular risk. While approximately 20 % of the population has an Lp(a) level greater than 50 mg/dL, there are no currently available pharmacological lipid-lowering therapies that have demonstrated substantial reduction in Lp(a). Novel therapies to lower Lp(a) include antisense oligonucleotides and small-interfering ribonucleic acid molecules and have shown promising results in phase 2 trials. Phase 3 trials are currently underway and will test the causal relationship between Lp(a) and ASCVD and whether lowering Lp(a) reduces cardiovascular outcomes. In this review, we summarize emerging insights related to Lp(a)'s role as a risk-enhancing factor for ASCVD, association with calcific aortic stenosis, effects of existing therapies on Lp(a) levels, and variations amongst patient populations. The evolving therapeutic landscape of emerging therapeutics is further discussed.
Keywords: Atherosclerotic cardiovascular disease; Calcific aortic stenosis; Dyslipidemia; Lipoprotein(a).
© 2024 The Authors. Published by Elsevier B.V.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: RB reports consulting/advisory fees from Amgen, and Novartis. MG reports consulting fees from BMS, Aepha, Horizon Therapeutics, Kiniksa Pharmaceuticals Corp. BW reports advisory/consulting from Novo Nordisk, BMS, Aepha, Horizon Therapeutics, and Kiniksa Pharmaceuticals.
Figures
References
-
- Berman A.N., Blankstein R. Current and future role of Lipoprotein(a) in preventive cardiology. Curr Opin Cardiol. 2019;34(5):514–518. - PubMed
-
- Varvel S., McConnell J.P., Tsimikas S. Prevalence of elevated Lp(a) mass levels and patient thresholds in 532 359 patients in the United States. Arterioscler Thromb Vasc Biol. 2016;36(11):2239–2245. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
