

The state of the art in the treatment of severe aplastic anemia: immunotherapy and hematopoietic cell transplantation in children and adults
- PMID: 38646536
- PMCID: PMC11026616
- DOI: 10.3389/fimmu.2024.1378432
The state of the art in the treatment of severe aplastic anemia: immunotherapy and hematopoietic cell transplantation in children and adults
Abstract
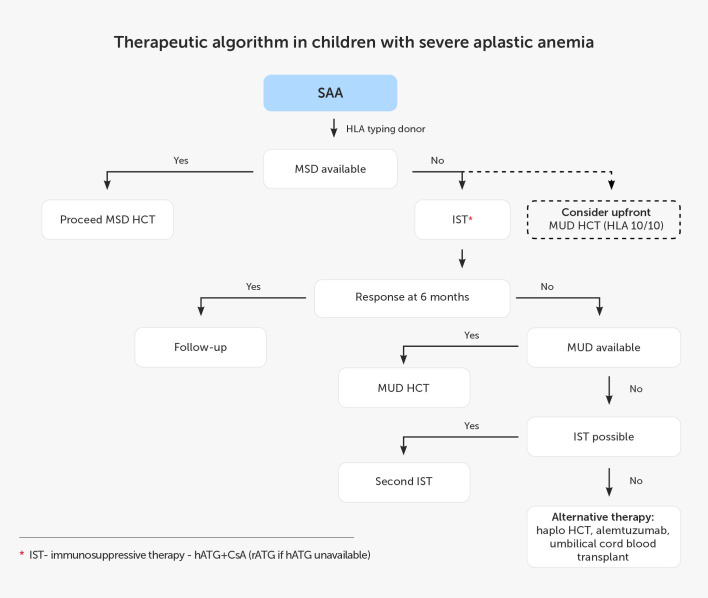
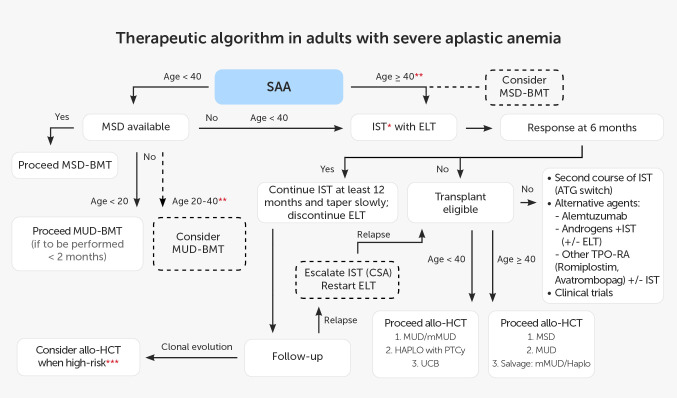
Acquired aplastic anemia (AA) is an immune-mediated bone marrow (BM) failure where marrow disruption is driven by a cytotoxic T-cell-mediated autoimmune attack against hematopoietic stem cells. The key diagnostic challenge in children, but also in adults, is to exclude the possible underlying congenital condition and myelodysplasia. The choice of treatment options, either allogeneic hematopoietic cell transplantation (alloHCT) or immunosuppressive therapy (IST), depends on the patient's age, comorbidities, and access to a suitable donor and effective therapeutic agents. Since 2022, horse antithymocyte globulin (hATG) has been available again in Europe and is recommended for IST as a more effective option than rabbit ATG. Therefore, an update on immunosuppressive strategies is warranted. Despite an improved response to the new immunosuppression protocols with hATG and eltrombopag, some patients are not cured or remain at risk of aplasia relapse or clonal evolution and require postponed alloHCT. The transplantation field has evolved, becoming safer and more accessible. Upfront alloHCT from unrelated donors is becoming a tempting option. With the use of posttransplant cyclophosphamide, haploidentical HCT offers promising outcomes also in AA. In this paper, we present the state of the art in the management of severe AA for pediatric and adult patients based on the available guidelines and recently published studies.
Keywords: antithymocyte globulin; aplastic anemia; eltrombopag; hATG; hematopoietic cell transplantation; immunosuppression; rATG.
Copyright © 2024 Piekarska, Pawelec, Szmigielska-Kapłon and Ussowicz.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Locasciulli A, Bacigalupo A, Bruno B, Montante B, Marsh J, Tichelli A, et al. Hepatitis-associated aplastic anaemia: epidemiology and treatment results obtained in Europe. A report of The EBMT aplastic anaemia working party. Br J Haematol. (2010) 149:890–5. doi: 10.1111/j.1365-2141.2010.08194.x - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical