

Mechanisms of ischaemia-induced arrhythmias in hypertrophic cardiomyopathy: a large-scale computational study
- PMID: 38646743
- PMCID: PMC11218689
- DOI: 10.1093/cvr/cvae086
Mechanisms of ischaemia-induced arrhythmias in hypertrophic cardiomyopathy: a large-scale computational study
Abstract
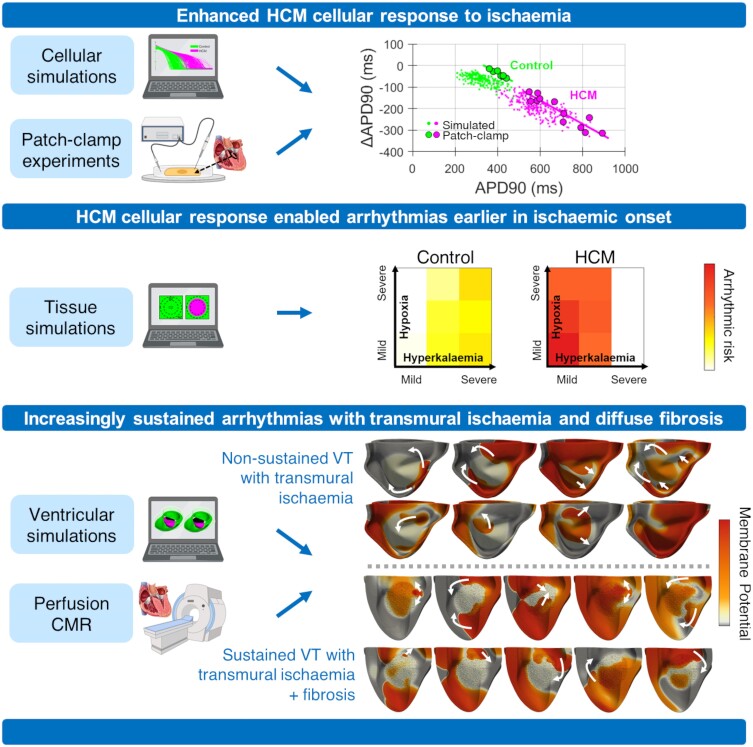
Aims: Lethal arrhythmias in hypertrophic cardiomyopathy (HCM) are widely attributed to myocardial ischaemia and fibrosis. How these factors modulate arrhythmic risk remains largely unknown, especially as invasive mapping protocols are not routinely used in these patients. By leveraging multiscale digital twin technologies, we aim to investigate ischaemic mechanisms of increased arrhythmic risk in HCM.
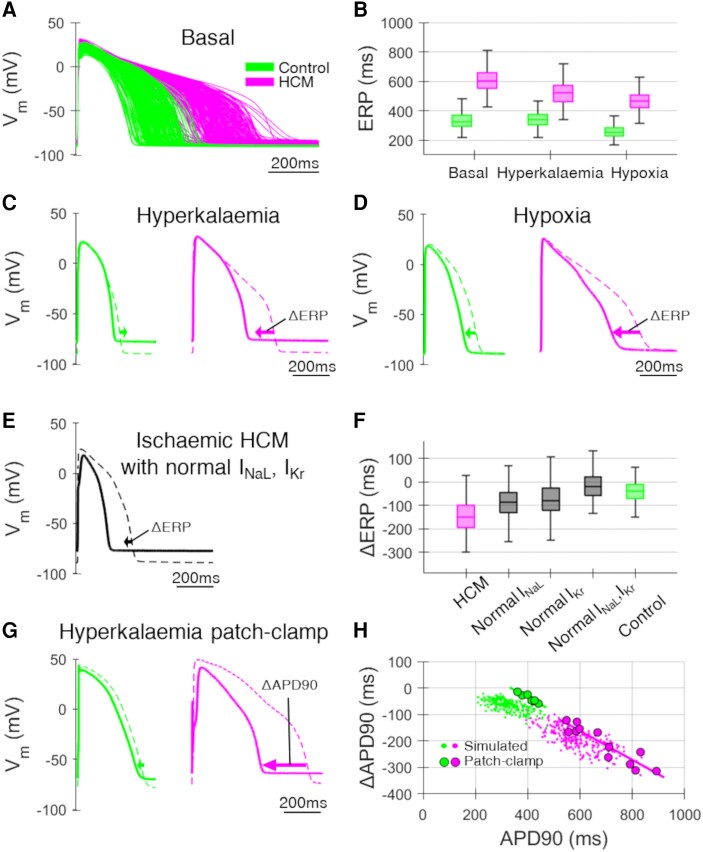
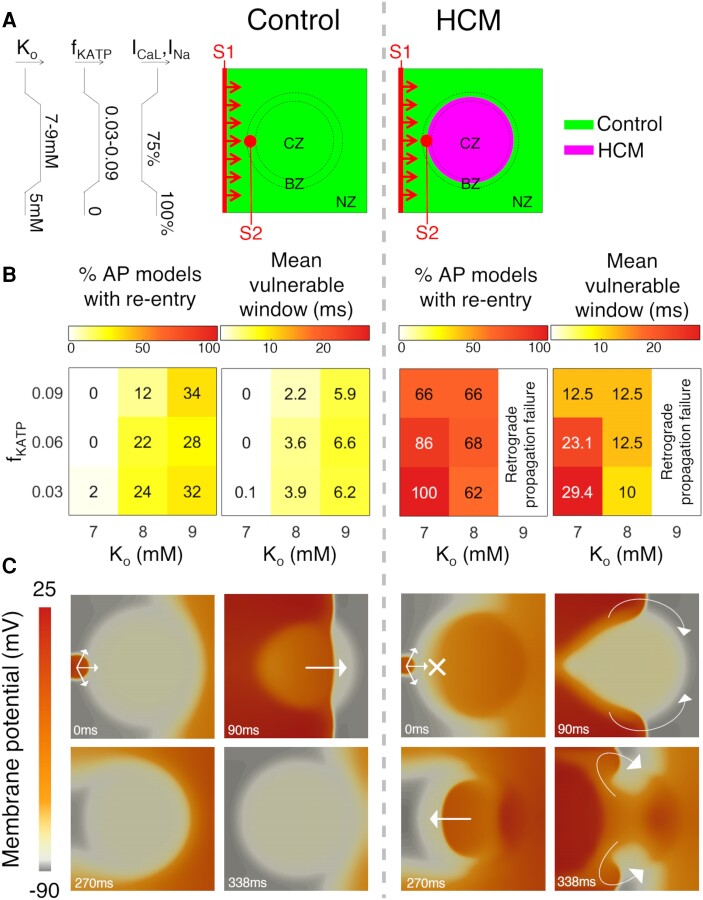
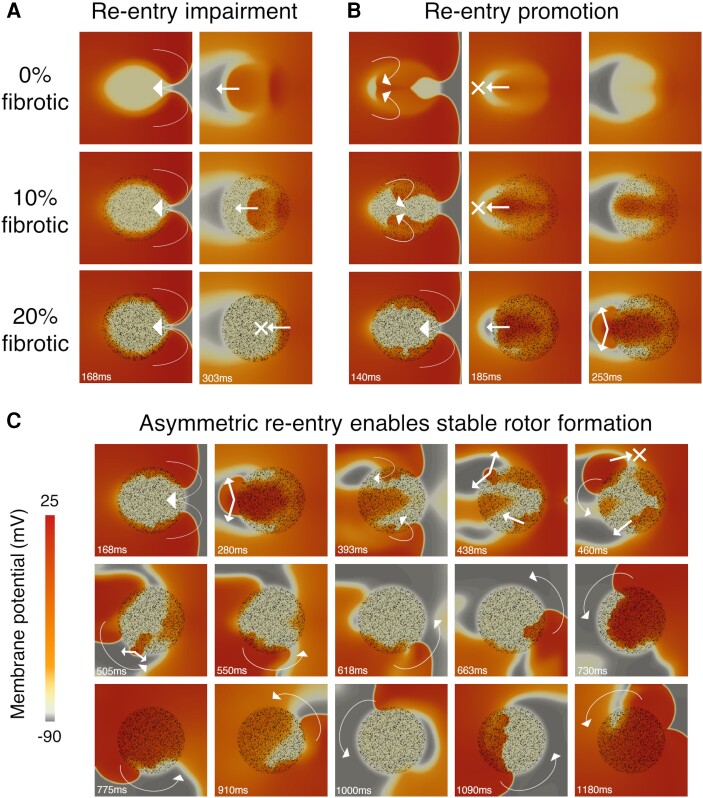
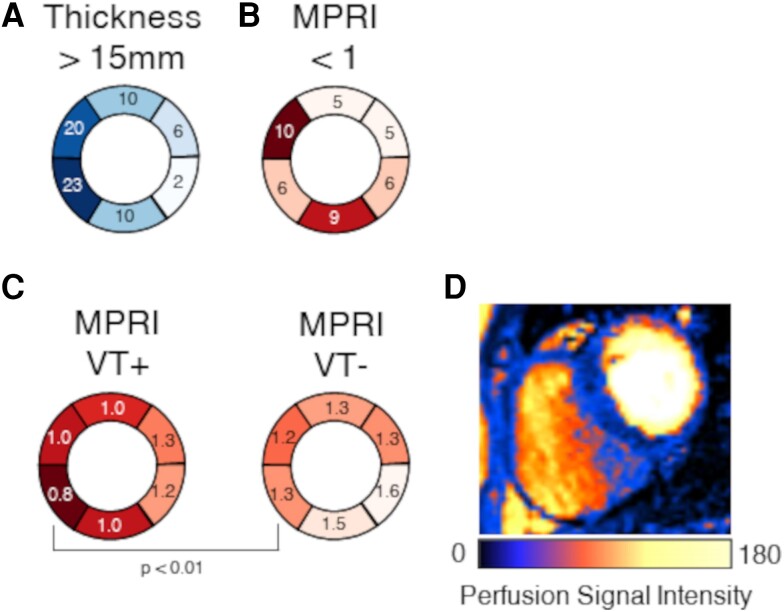
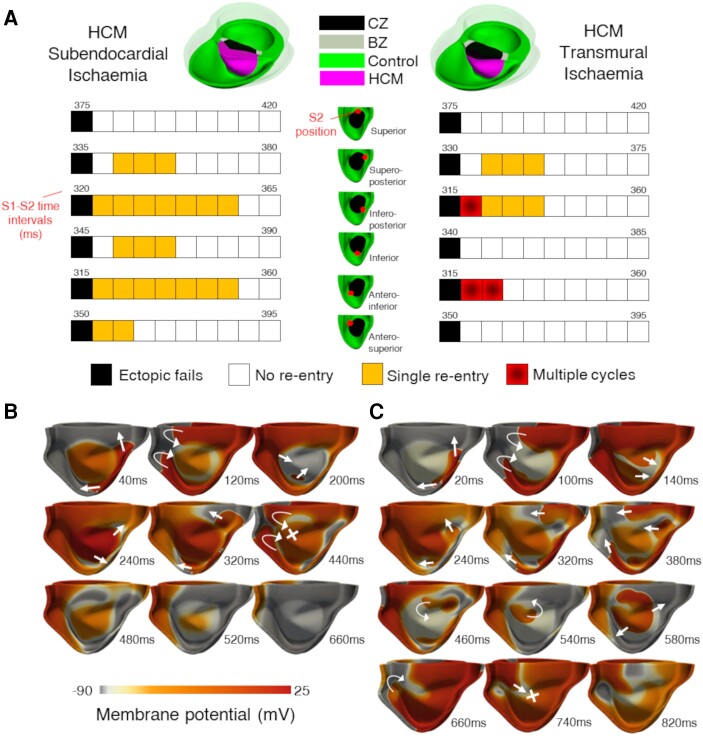
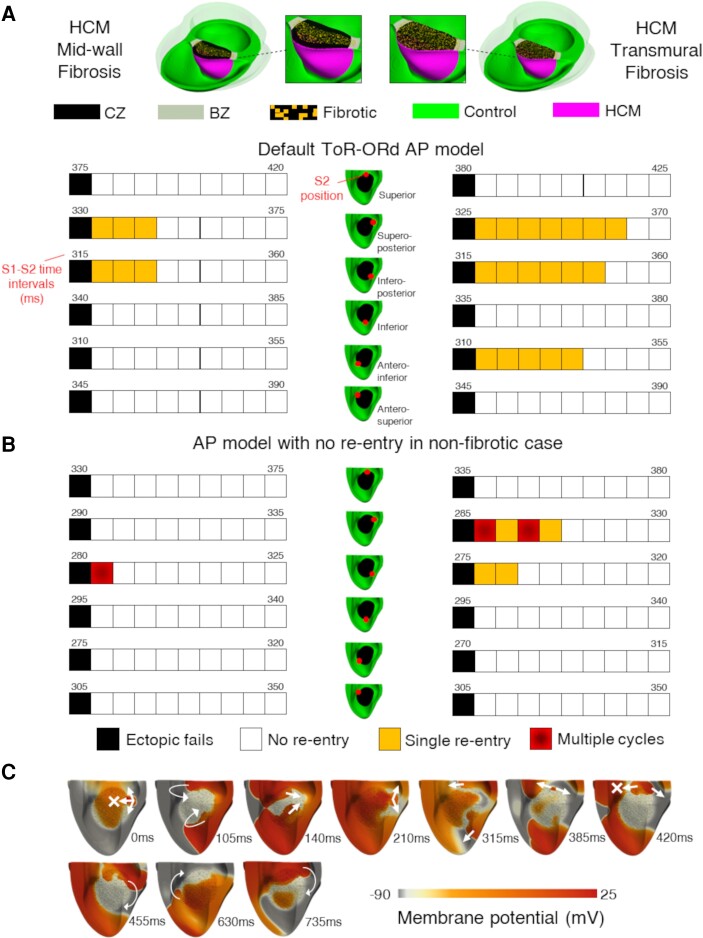
Methods and results: Computational models of human HCM cardiomyocytes, tissue, and ventricles were used to simulate outcomes of Phase 1A acute myocardial ischaemia. Cellular response predictions were validated with patch-clamp studies of human HCM cardiomyocytes (n = 12 cells, N = 5 patients). Ventricular simulations were informed by typical distributions of subendocardial/transmural ischaemia as analysed in perfusion scans (N = 28 patients). S1-S2 pacing protocols were used to quantify arrhythmic risk for scenarios in which regions of septal obstructive hypertrophy were affected by (i) ischaemia, (ii) ischaemia and impaired repolarization, and (iii) ischaemia, impaired repolarization, and diffuse fibrosis. HCM cardiomyocytes exhibited enhanced action potential and abnormal effective refractory period shortening to ischaemic insults. Analysis of ∼75 000 re-entry induction cases revealed that the abnormal HCM cellular response enabled establishment of arrhythmia at milder ischaemia than otherwise possible in healthy myocardium, due to larger refractoriness gradients that promoted conduction block. Arrhythmias were more easily sustained in transmural than subendocardial ischaemia. Mechanisms of ischaemia-fibrosis interaction were strongly electrophysiology dependent. Fibrosis enabled asymmetric re-entry patterns and break-up into sustained ventricular tachycardia.
Conclusion: HCM ventricles exhibited an increased risk to non-sustained and sustained re-entry, largely dominated by an impaired cellular response and deleterious interactions with the diffuse fibrotic substrate.
Keywords: Arrhythmic risk; Hypertrophic cardiomyopathy; Ischaemia; Modelling and simulation.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: none declared.
Figures
Similar articles
-
Similar arrhythmicity in hypertrophic and fibrotic cardiac cultures caused by distinct substrate-specific mechanisms.Cardiovasc Res. 2013 Jan 1;97(1):171-81. doi: 10.1093/cvr/cvs290. Epub 2012 Sep 12. Cardiovasc Res. 2013. PMID: 22977008
-
Mechanisms of pro-arrhythmic abnormalities in ventricular repolarisation and anti-arrhythmic therapies in human hypertrophic cardiomyopathy.J Mol Cell Cardiol. 2016 Jul;96:72-81. doi: 10.1016/j.yjmcc.2015.09.003. Epub 2015 Sep 16. J Mol Cell Cardiol. 2016. PMID: 26385634 Free PMC article.
-
Cardiovascular magnetic resonance T2* mapping for the assessment of cardiovascular events in hypertrophic cardiomyopathy.Open Heart. 2020 Mar 15;7(1):e001152. doi: 10.1136/openhrt-2019-001152. eCollection 2020. Open Heart. 2020. PMID: 32201584 Free PMC article.
-
Abnormalities in sodium current and calcium homoeostasis as drivers of arrhythmogenesis in hypertrophic cardiomyopathy.Cardiovasc Res. 2020 Jul 15;116(9):1585-1599. doi: 10.1093/cvr/cvaa124. Cardiovasc Res. 2020. PMID: 32365196 Review.
-
Mechanisms and prognostic impact of myocardial ischaemia in hypertrophic cardiomyopathy.Int J Cardiovasc Imaging. 2023 Oct;39(10):1979-1996. doi: 10.1007/s10554-023-02894-y. Epub 2023 Jun 26. Int J Cardiovasc Imaging. 2023. PMID: 37358707 Free PMC article. Review.
Cited by
-
The Role of Signalling Pathways in Myocardial Fibrosis in Hypertrophic Cardiomyopathy.Rev Cardiovasc Med. 2025 Feb 21;26(2):27152. doi: 10.31083/RCM27152. eCollection 2025 Feb. Rev Cardiovasc Med. 2025. PMID: 40026508 Free PMC article. Review.
-
Storytelling of Hypertrophic Cardiomyopathy Discovery.J Cardiovasc Dev Dis. 2024 Sep 28;11(10):300. doi: 10.3390/jcdd11100300. J Cardiovasc Dev Dis. 2024. PMID: 39452271 Free PMC article. Review.
References
-
- Maron MS, Rowin EJ, Wessler BS, Mooney PJ, Fatima A, Patel P, Koethe BC, Romashko M, Link MS, Maron BJ. Enhanced American College of Cardiology/American Heart Association strategy for prevention of sudden cardiac death in high-risk patients with hypertrophic cardiomyopathy. J Am Coll Cardiol 2019;4:644–657. - PMC - PubMed
-
- Arbelo E, Protonotarios A, Gimeno JR, Arbustini E, Barriales-Villa R, Basso C, Bezzina CR, Biagini E, Blom NA, de Boer RA, De Winter T, Elliott PM, Flather M, Garcia-Pavia P, Haugaa KH, Ingles J, Jurcut RO, Klaassen S, Limongelli G, Loeys B, Mogensen J, Olivotto I, Pantazis A, Sharma S, Van Tintelen JP, Ware JS, Kaski JP, ESC Scientific Document Group . 2023 ESC Guidelines for the management of cardiomyopathies: developed by the task force on the management of cardiomyopathies of the European Society of Cardiology (ESC). Eur Heart J 2023;44:3503–3626. - PubMed
-
- Conway J, Min S, Villa C, Weintraub RG, Nakano S, Godown J, Tatangelo M, Armstrong K, Richmond M, Kaufman B, Lal AK, Balaji S, Power A, Baez Hernandez N, Gardin L, Kantor PF, Parent JJ, Aziz PF, Jefferies JL, Dragulescu A, Jeewa A, Benson L, Russell MW, Whitehill R, Rossano J, Howard T, Mital S. The prevalence and association of exercise test abnormalities with sudden cardiac death and transplant-free survival in childhood hypertrophic cardiomyopathy. Circulation 2022;147:718–727. - PMC - PubMed
-
- Wu VC-C, Chen T-H, Wu M, Chen S-W, Chang C-H, Chang C-W, Chen C-C, Wu KP-H, Hsieh M-J, Wang C-Y, Chang S-H, Lin F-C, Hsieh I-C, Chu P-H, Wen M-S. Outcomes of patients with hypertrophic cardiomyopathy and acute myocardial infarction: a propensity score-matched, 15-year nationwide population-based study in Asia. BMJ Open 2018;8:e019741. - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
