

Motor band sign is specific for amyotrophic lateral sclerosis and corresponds to motor symptoms
- PMID: 38647181
- PMCID: PMC11093233
- DOI: 10.1002/acn3.52066
Motor band sign is specific for amyotrophic lateral sclerosis and corresponds to motor symptoms
Abstract
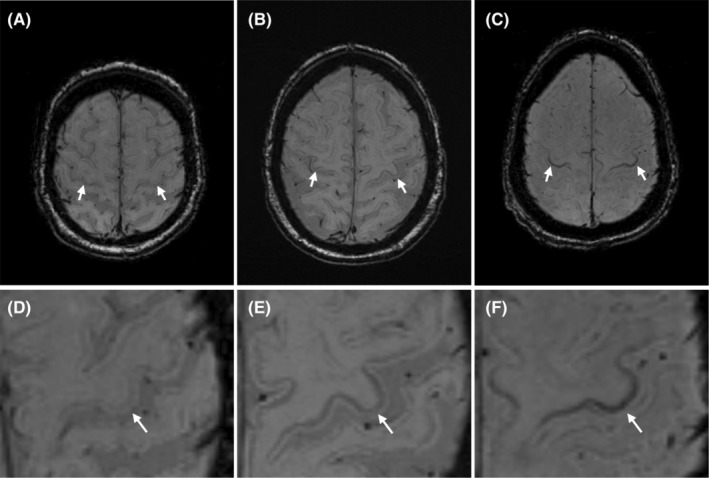
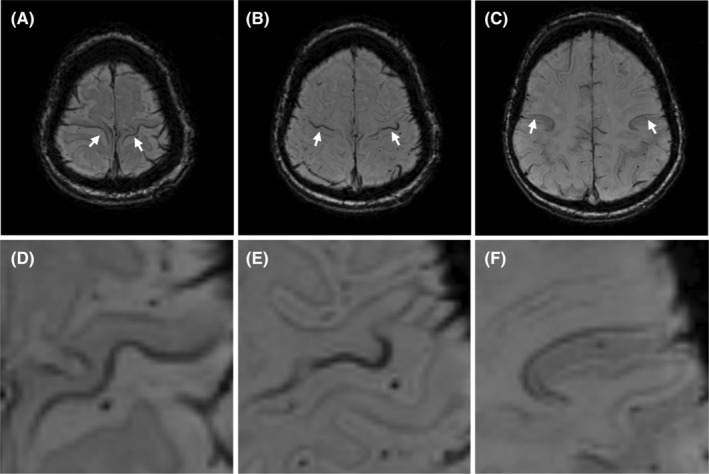
Objective: Magnetic resonance imaging can detect neurodegenerative iron accumulation in the motor cortex, called the motor band sign. This study aims to evaluate its sensitivity/specificity and correlations to symptomatology, biomarkers, and clinical outcome in amyotrophic lateral sclerosis.
Methods: This prospective study consecutively enrolled 114 persons with amyotrophic lateral sclerosis and 79 mimics referred to Karolinska University Hospital, and also 31 healthy controls. All underwent 3-Tesla brain susceptibility-weighted imaging. Three raters independently assessed motor cortex susceptibility with total and regional motor band scores. Survival was evaluated at a median of 34.2 months after the imaging.
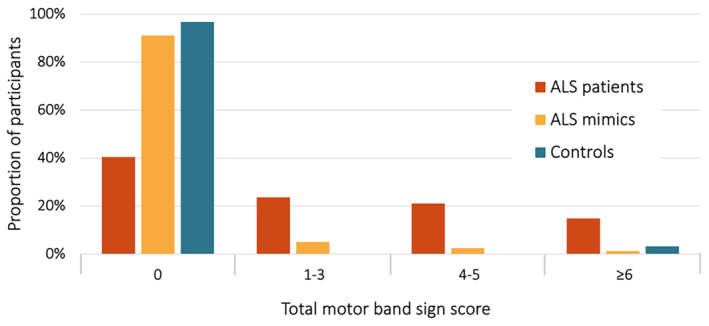
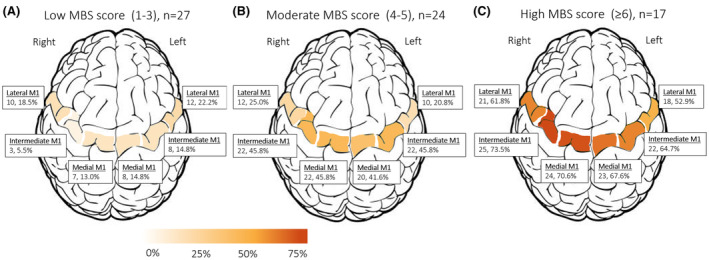
Results: The motor band sign identified amyotrophic lateral sclerosis with a sensitivity of 59.6% and a specificity of 91.1% versus mimics and 96.8% versus controls. Higher motor band scores were more common with genetic risk factors (p = 0.032), especially with C9orf72 mutation, and were associated with higher neurofilament light levels (std. β 0.22, p = 0.019). Regional scores correlated strongly with focal symptoms (medial region vs. gross motor dysfunction, std. β -0.64, p = 0.001; intermediate region vs. fine motor dysfunction, std. β -0.51, p = 0.031; lateral region vs. bulbar symptoms std. β -0.71, p < 0.001). There were no associations with cognition, progression rate, or survival.
Interpretation: In a real-life clinical setting, the motor band sign has high specificity but relatively low sensitivity for identifying amyotrophic lateral sclerosis. Associations with genetic risk factors, neurofilament levels and somatotopic correspondence to focal motor weakness suggest that the motor band sign could be a suitable biomarker for diagnostics and clinical trials in amyotrophic lateral sclerosis.
© 2024 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
C.I. has consulted for Cytokinetics, Pfizer, BioArctic, Novartis, Tikomed, Ferrer, and Mitsubishi. She is also a DMC member for Appelis, a Pharmaceutical Board member of Tobii Dynavox and Stiching, and a Scientific Advisory council member for the international Alliance. There are no other conflicts of interest to declare.
Figures
Similar articles
-
Brain signal intensity changes as biomarkers in amyotrophic lateral sclerosis.Acta Neurol Scand. 2018 Feb;137(2):262-271. doi: 10.1111/ane.12863. Epub 2017 Oct 29. Acta Neurol Scand. 2018. PMID: 29082510
-
Amyotrophic lateral sclerosis with upper motor neuron predominance: diagnostic accuracy of qualitative and quantitative susceptibility metrics in the precentral gyrus.Eur Radiol. 2023 Nov;33(11):7677-7685. doi: 10.1007/s00330-023-10070-y. Epub 2023 Aug 22. Eur Radiol. 2023. PMID: 37606662
-
Semiautomated Evaluation of the Primary Motor Cortex in Patients with Amyotrophic Lateral Sclerosis at 3T.AJNR Am J Neuroradiol. 2018 Jan;39(1):63-69. doi: 10.3174/ajnr.A5423. Epub 2017 Nov 9. AJNR Am J Neuroradiol. 2018. PMID: 29122765 Free PMC article.
-
Biomarker discovery and development for frontotemporal dementia and amyotrophic lateral sclerosis.Brain. 2022 Jun 3;145(5):1598-1609. doi: 10.1093/brain/awac077. Brain. 2022. PMID: 35202463 Free PMC article. Review.
-
The motor cortex and amyotrophic lateral sclerosis.Muscle Nerve. 2001 Apr;24(4):564-73. doi: 10.1002/mus.1042. Muscle Nerve. 2001. PMID: 11268031 Review.
Cited by
-
Blood diagnostic and prognostic biomarkers in amyotrophic lateral sclerosis.Neural Regen Res. 2025 Sep 1;20(9):2556-2570. doi: 10.4103/NRR.NRR-D-24-00286. Epub 2024 Sep 24. Neural Regen Res. 2025. PMID: 39314138 Free PMC article.
-
sTREM2 cerebrospinal fluid levels are a potential biomarker in amyotrophic lateral sclerosis and associate with UMN burden.Front Neurol. 2024 Dec 10;15:1515252. doi: 10.3389/fneur.2024.1515252. eCollection 2024. Front Neurol. 2024. PMID: 39722698 Free PMC article.
References
-
- Ringholz GM, Appel SH, Bradshaw M, Cooke NA, Mosnik DM, Schulz PE. Prevalence and patterns of cognitive impairment in sporadic ALS. Neurology. 2005;65(4):586‐590. - PubMed
-
- Sennfält S, Kläppe U, Thams S, et al. The path to diagnosis in ALS: Delay, referrals, alternate diagnoses, and clinical progression. Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration. 2023;24(1‐2):45‐53. - PubMed
-
- Hannaford A, Pavey N, van den Bos M, et al. Diagnostic utility of Gold Coast criteria in amyotrophic lateral sclerosis. Ann Neurol. 2021;89(5):979‐986. - PubMed
-
- Brooks BR, Miller RG, Swash M, Munsat TL, World Federation of Neurology Research Group on Motor Neuron Diseases . El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord. 2000;1(5):293‐299. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials