

Reducing Firearm Access for Suicide Prevention: Implementation Evaluation of the Web-Based "Lock to Live" Decision Aid in Routine Health Care Encounters
- PMID: 38647319
- PMCID: PMC11063417
- DOI: 10.2196/48007
Reducing Firearm Access for Suicide Prevention: Implementation Evaluation of the Web-Based "Lock to Live" Decision Aid in Routine Health Care Encounters
Abstract
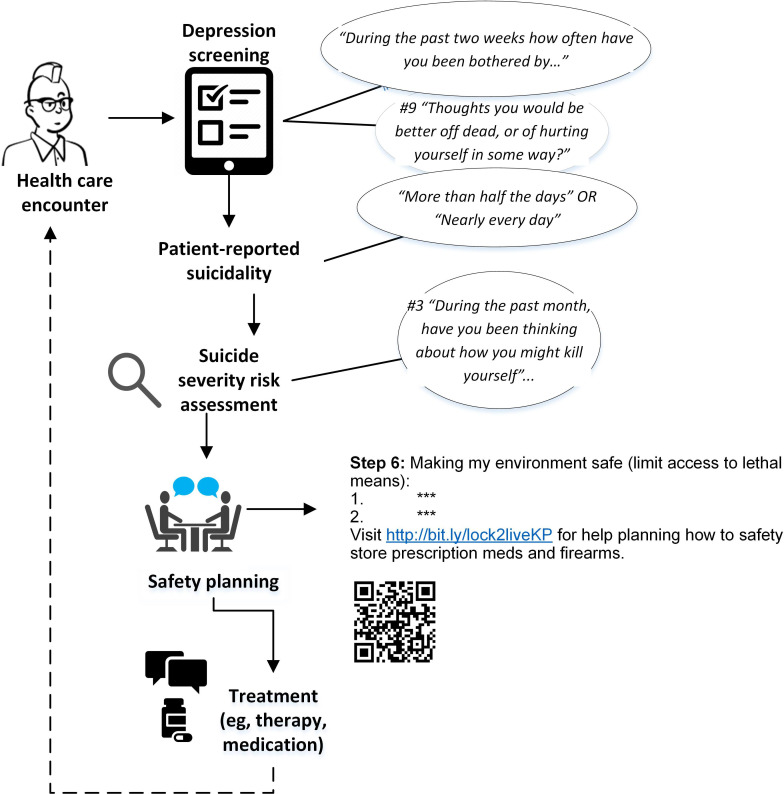
Background: "Lock to Live" (L2L) is a novel web-based decision aid for helping people at risk of suicide reduce access to firearms. Researchers have demonstrated that L2L is feasible to use and acceptable to patients, but little is known about how to implement L2L during web-based mental health care and in-person contact with clinicians.
Objective: The goal of this project was to support the implementation and evaluation of L2L during routine primary care and mental health specialty web-based and in-person encounters.
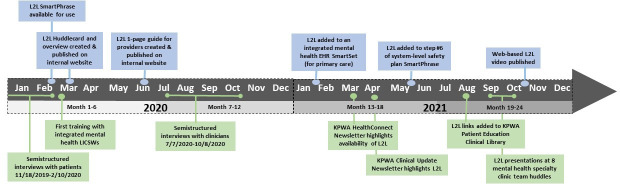
Methods: The L2L implementation and evaluation took place at Kaiser Permanente Washington (KPWA)-a large, regional, nonprofit health care system. Three dimensions from the RE-AIM (Reach, Effectiveness, Adoption, Implementation, Maintenance) model-Reach, Adoption, and Implementation-were selected to inform and evaluate the implementation of L2L at KPWA (January 1, 2020, to December 31, 2021). Electronic health record (EHR) data were used to purposefully recruit adult patients, including firearm owners and patients reporting suicidality, to participate in semistructured interviews. Interview themes were used to facilitate L2L implementation and inform subsequent semistructured interviews with clinicians responsible for suicide risk mitigation. Audio-recorded interviews were conducted via the web, transcribed, and coded, using a rapid qualitative inquiry approach. A descriptive analysis of EHR data was performed to summarize L2L reach and adoption among patients identified at high risk of suicide.
Results: The initial implementation consisted of updates for clinicians to add a URL and QR code referencing L2L to the safety planning EHR templates. Recommendations about introducing L2L were subsequently derived from the thematic analysis of semistructured interviews with patients (n=36), which included (1) "have an open conversation," (2) "validate their situation," (3) "share what to expect," (4) "make it accessible and memorable," and (5) "walk through the tool." Clinicians' interviews (n=30) showed a strong preference to have L2L included by default in the EHR-based safety planning template (in contrast to adding it manually). During the 2-year observation period, 2739 patients reported prior-month suicide attempt planning or intent and had a documented safety plan during the study period, including 745 (27.2%) who also received L2L. Over four 6-month subperiods of the observation period, L2L adoption rates increased substantially from 2% to 29% among primary care clinicians and from <1% to 48% among mental health clinicians.
Conclusions: Understanding the value of L2L from users' perspectives was essential for facilitating implementation and increasing patient reach and clinician adoption. Incorporating L2L into the existing system-level, EHR-based safety plan template reduced the effort to use L2L and was likely the most impactful implementation strategy. As rising suicide rates galvanize the urgency of prevention, the findings from this project, including L2L implementation tools and strategies, will support efforts to promote safety for suicide prevention in health care nationwide.
Keywords: decision aid; electronic health record; evaluation; feasible; firearm; implementation; internet; mental health; prevention; risk; suicide; suicide prevention; support; tool.
© Julie Elissa Richards, Elena Kuo, Christine Stewart, Lisa Shulman, Rebecca Parrish, Ursula Whiteside, Jennifer M Boggs, Gregory E Simon, Ali Rowhani-Rahbar, Marian E Betz. Originally published in JMIR Medical Informatics (https://medinform.jmir.org).
Conflict of interest statement
Figures
Similar articles
-
Patient and Clinician Perspectives of a Standardized Question About Firearm Access to Support Suicide Prevention: A Qualitative Study.JAMA Health Forum. 2022 Nov 4;3(11):e224252. doi: 10.1001/jamahealthforum.2022.4252. JAMA Health Forum. 2022. PMID: 36416815 Free PMC article.
-
An Interactive Web-Based Lethal Means Safety Decision Aid for Suicidal Adults (Lock to Live): Pilot Randomized Controlled Trial.J Med Internet Res. 2020 Jan 29;22(1):e16253. doi: 10.2196/16253. J Med Internet Res. 2020. PMID: 32012056 Free PMC article. Clinical Trial.
-
"Lock to Live" for firearm and medication safety: Feasibility and acceptability of a suicide prevention tool in a learning healthcare system.Front Digit Health. 2022 Sep 6;4:974153. doi: 10.3389/fdgth.2022.974153. eCollection 2022. Front Digit Health. 2022. PMID: 36148209 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Examining Home Visits from Community Health Workers to Help Patients Manage Asthma Symptoms [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Dec. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Dec. PMID: 37874896 Free Books & Documents. Review.
References
-
- WISQARS — your source for U.S. injury statistics. Centers for Disease Control and Prevention. [26-04-2022]. https://www.cdc.gov/injury/wisqars/facts.html URL. Accessed.
-
- McCracken H, Okuley H, Floyd L. Gun ownership in America. RAND Corporation. [10-01-2022]. https://www.rand.org/research/gun-policy/gun-ownership.html URL. Accessed.
-
- Parker K, Horowitz JM, Igielnik R, Oliphant JB, Brown A. America’s complex relationship with guns. Pew Research Center. Jun 22, 2017. [29-03-2022]. https://www.pewresearch.org/social-trends/2017/06/22/americas-complex-re... URL. Accessed.
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
