

Curative resection via right hemicolectomy and regional lymph node dissection for colonic adenomatous polyposis of unknown etiology with adenocarcinomas localized in the right side of the colon: a case report
- PMID: 38647838
- PMCID: PMC11035501
- DOI: 10.1186/s40792-024-01890-1
Curative resection via right hemicolectomy and regional lymph node dissection for colonic adenomatous polyposis of unknown etiology with adenocarcinomas localized in the right side of the colon: a case report
Abstract
Background: APC and MUTYH are both well-known colorectal polyposis causative genes. However, 30-50% of colorectal adenomatous polyposis cases are classified as colonic adenomatous polyposis of unknown etiology and lack identifiable pathogenic variants. Although guidelines recommend total proctocolectomy for colonic adenomatous polyposis of unknown etiology with over 100 adenomas, evidence is lacking. This study presents a unique case of localized colonic adenomatous polyposis of unknown etiology with multiple adenocarcinomas, treated with hemicolectomy and regional lymph node dissection.
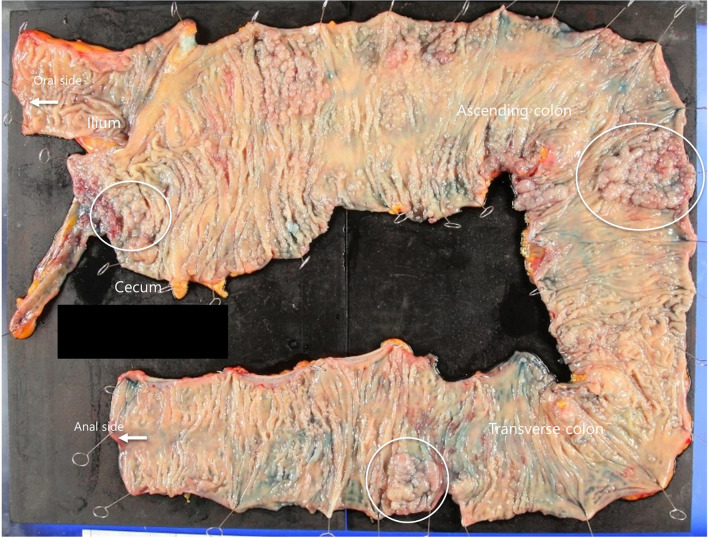
Case presentation: The patient was a 72-year-old woman whose colonoscopy revealed numerous polyps and two adenocarcinomas localized in the right side of the colon, with no lesions in the left side. The patient had no family history of polyposis or colorectal cancer. No extracolonic lesions, enlarged lymph nodes, or distant metastases were found. Considering the patient's age and lesion localization, laparoscopic right hemicolectomy with regional lymph node dissection was performed. Histopathological diagnosis revealed three adenocarcinoma lesions with no lymph node metastasis. The most advanced pathological stage was T2N0M0 Stage I (UICC 8th edition). The patient was alive 5 years postoperatively, without recurrence of cancer or polyposis in the remaining colon and rectum. To diagnose hereditary colorectal cancer/polyposis, a germline multigene panel testing for APC, EPCAM, MBD4, MLH1, MLH3, MSH2, MSH3, MSH6, MUTYH, NTHL1, PMS2, POLD1, POLE, and TP53 was performed using DNA extracted from blood samples: however, no pathogenic variant was detected. Therefore, the patient was diagnosed with colonic adenomatous polyposis of unknown etiology.
Conclusions: In this rare case, colonic adenomatous polyposis of unknown etiology, with numerous adenomatous polyps and multiple adenocarcinomas localized in the right side of the colon, was successfully treated with right hemicolectomy and regional lymph node dissection. Despite genetic analysis, no causative germline variants were identified. Segmental colectomy according to the distribution of polyps might be a curative approach.
Keywords: MSH3; Colonic adenomatous polyposis of unknown etiology; Colorectal cancer.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Horpaopan S, Spier I, Zink AM, Altmüller J, Holzapfel S, Laner A, et al. Genome-wide CNV analysis in 221 unrelated patients and targeted high-throughput sequencing reveal novel causative candidate genes for colorectal adenomatous polyposis. Int J Cancer. 2015;136:E578–E589. doi: 10.1002/ijc.29215. - DOI - PubMed
-
- Weiss JM, Gupta S, Burke CA, Axell L, Chen LM, Chung DC, et al. NCCN guidelines® insights: genetic/familial high-risk assessment: colorectal, version 1.2021. J Natl Compr Canc Netw. 2021;19:1122–1132. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
