

Selpercatinib for treating recurrent mixed medullary and follicular cell-derived thyroid carcinoma: a case report
- PMID: 38647958
- PMCID: PMC11035533
- DOI: 10.1186/s40792-024-01898-7
Selpercatinib for treating recurrent mixed medullary and follicular cell-derived thyroid carcinoma: a case report
Abstract
Background: Mixed medullary and follicular cell-derived thyroid carcinoma (MMFCC) is characterized by the coexistence of follicular and C cell-derived tumour cell populations within the same lesion. Due to its rarity, its etiology and clinical course remain unclear, and treatment for advanced or recurrent cases has not been established.
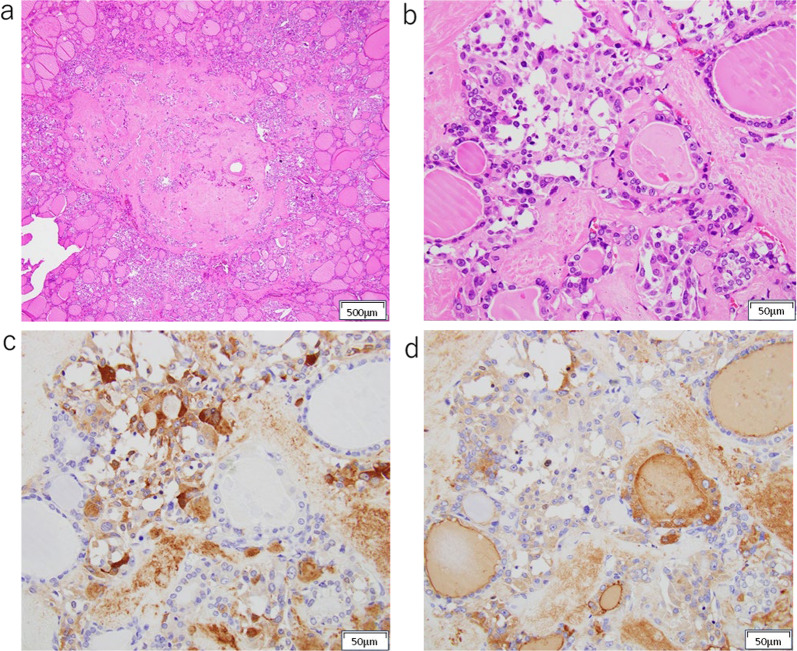
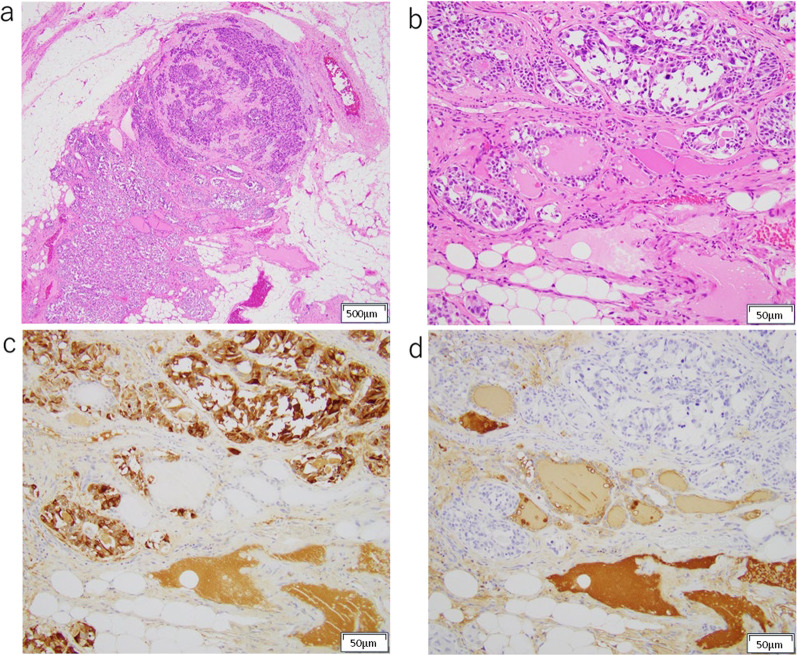
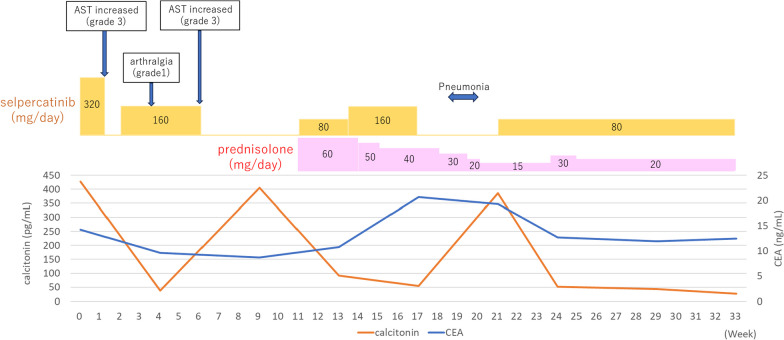
Case presentation: We report a case of MMFCC treated with selpercatinib. The patient was a 69-year-old male presenting with tumors in the right thyroid lobe and in the upper mediastinum. Fine-needle aspiration (FNA) cytology of the right thyroid lobe tumor revealed a medullary carcinoma; germline RET mutations were not detected. After resection of the right thyroid lobe with central node dissection, rapid intraoperative diagnosis of the mediastinal mass confirmed malignancy, leading to total thyroidectomy with excision of the upper mediastinal tumor. Histologically, the tumor in the right thyroid lobe and the pretracheal lymph node revealed a mixture of medullary and follicular carcinoma components, diagnosed as MMFCC. The mediastinal lymph node exhibited only medullary carcinoma components. At 11 months postoperatively, computed tomography scans showed enlargement of the right supraclavicular and upper mediastinal lymph nodes. FNA cytology of the right supraclavicular lymph node suggested the recurrence of medullary thyroid carcinoma. The gene panel testing (The Oncomine Dx Target Test Multi-CDx system®, Thermo Fisher SCIENTIFIC) of metastatic lymph node revealed RET somatic mutation (M918T). Treatment with selpercatinib was initiated, and both the cervical and mediastinal lymph nodes showed a reduction in size.
Conclusions: We report a rare case of selpercatinib use for MMFCC. Since RET mutations may occur frequently in MMFCC, selpercatinib could be effective in treating MMFCC.
Keywords: RET mutation; Mixed medullary and follicular cell-derived thyroid carcinoma; Selpercatinib.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
Multiple Endocrine Neoplasia Type 2B Associated Mixed Medullary and Follicular Thyroid Carcinoma in A Chinese Patient with RET M918T Germline Mutation.Endocr Metab Immune Disord Drug Targets. 2021;21(3):554-560. doi: 10.2174/1871530320666200713092633. Endocr Metab Immune Disord Drug Targets. 2021. PMID: 32660411
-
Neoadjuvant Chemotherapy With Selpercatinib for Locally Advanced RET Fusion-Positive Papillary Thyroid Carcinoma: A Case Report.Case Rep Endocrinol. 2025 Jun 3;2025:6676471. doi: 10.1155/crie/6676471. eCollection 2025. Case Rep Endocrinol. 2025. PMID: 40496634 Free PMC article.
-
Mixed medullary-papillary carcinoma of the thyroid: report of a case and review of the literature.Head Neck. 2009 Jul;31(7):968-74. doi: 10.1002/hed.20984. Head Neck. 2009. PMID: 19260112 Review.
-
Rapid and long-lasting response to selpercatinib of paraneoplastic Cushing's syndrome in medullary thyroid carcinoma.Eur Thyroid J. 2022 Sep 28;11(6):e220032. doi: 10.1530/ETJ-22-0032. Print 2022 Dec 1. Eur Thyroid J. 2022. PMID: 36069795 Free PMC article.
-
The role of molecular testing in the diagnosis of medullary thyroid cancer: A case report of oncocytic medullary thyroid carcinoma and review of the literature.Am J Otolaryngol. 2020 Jan-Feb;41(1):102312. doi: 10.1016/j.amjoto.2019.102312. Epub 2019 Nov 11. Am J Otolaryngol. 2020. PMID: 31727331 Review.
Cited by
-
Histopathology of C Cells and Medullary Thyroid Carcinoma.Recent Results Cancer Res. 2025;223:9-50. doi: 10.1007/978-3-031-80396-3_2. Recent Results Cancer Res. 2025. PMID: 40102253 Review.
-
Limited Thyroidectomy Achieves Equivalent Survival to Total Thyroidectomy for Early Localized Medullary Thyroid Cancer.Cancers (Basel). 2024 Dec 4;16(23):4062. doi: 10.3390/cancers16234062. Cancers (Basel). 2024. PMID: 39682246 Free PMC article.
-
Adverse event profiles of selpercatinib: a real-world pharmacovigilance analysis based on FAERS database.BMC Cancer. 2024 Dec 3;24(1):1486. doi: 10.1186/s12885-024-13250-1. BMC Cancer. 2024. PMID: 39627756 Free PMC article.
-
A Malignant Duo: Mixed Medullary and Follicular Variant Papillary Thyroid Cancer.Cureus. 2024 Aug 19;16(8):e67231. doi: 10.7759/cureus.67231. eCollection 2024 Aug. Cureus. 2024. PMID: 39295705 Free PMC article.
References
LinkOut - more resources
Full Text Sources
