

Prevalence of Homologous Recombination Deficiency Among Patients With Germline RAD51C/D Breast or Ovarian Cancer
- PMID: 38648056
- PMCID: PMC11036141
- DOI: 10.1001/jamanetworkopen.2024.7811
Prevalence of Homologous Recombination Deficiency Among Patients With Germline RAD51C/D Breast or Ovarian Cancer
Abstract
Importance: RAD51C and RAD51D are involved in DNA repair by homologous recombination. Germline pathogenic variants (PVs) in these genes are associated with an increased risk of ovarian and breast cancer. Understanding the homologous recombination deficiency (HRD) status of tumors from patients with germline PVs in RAD51C/D could guide therapeutic decision-making and improve survival.
Objective: To characterize the clinical and tumor characteristics of germline RAD51C/D PV carriers, including the evaluation of HRD status.
Design, setting, and participants: This retrospective cohort study included 91 index patients plus 90 relatives carrying germline RAD51C/D PV (n = 181) in Spanish hospitals from January 1, 2014, to December 31, 2021. Genomic and functional HRD biomarkers were assessed in untreated breast and ovarian tumor samples (n = 45) from June 2022 to February 2023.
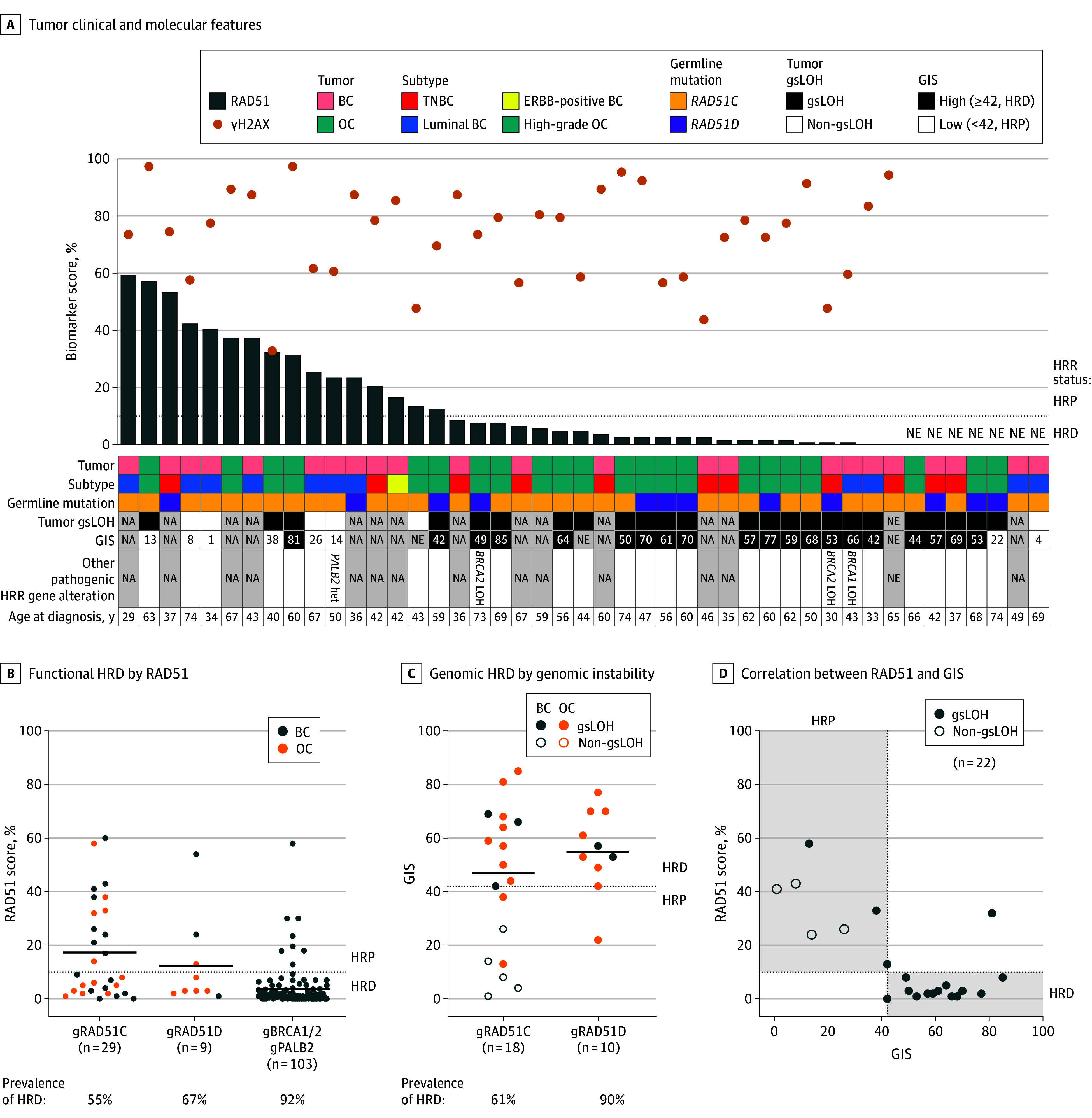
Main outcomes and measures: Clinical and pathologic characteristics were assessed using descriptive statistics. Genomic HRD by genomic instability scores, functional HRD by RAD51, and gene-specific loss of heterozygosity were analyzed. Associations between HRD status and tumor subtype, age at diagnosis, and gene-specific loss of heterozygosity in RAD51C/D were investigated using logistic regression or the t test.
Results: A total of 9507 index patients were reviewed, and 91 patients (1.0%) were found to carry a PV in RAD51C/D; 90 family members with a germline PV in RAD51C/D were also included. A total of 157 of carriers (86.7%) were women and 181 (55.8%) had received a diagnosis of cancer, mainly breast cancer or ovarian cancer. The most prevalent PVs were c.1026+5_1026+7del (11 of 56 [19.6%]) and c.709C>T (9 of 56 [16.1%]) in RAD51C and c.694C>T (20 of 35 [57.1%]) in RAD51D. In untreated breast cancer and ovarian cancer, the prevalence of functional and genomic HRD was 55.2% (16 of 29) and 61.1% (11 of 18) for RAD51C, respectively, and 66.7% (6 of 9) and 90.0% (9 of 10) for RAD51D. The concordance between HRD biomarkers was 91%. Tumors with the same PV displayed contrasting HRD status, and age at diagnosis did not correlate with the occurrence of HRD. All breast cancers retaining the wild-type allele were estrogen receptor positive and lacked HRD.
Conclusions and relevance: In this cohort study of germline RAD51C/D breast cancer and ovarian cancer, less than 70% of tumors displayed functional HRD, and half of those that did not display HRD were explained by retention of the wild-type allele, which was more frequent among estrogen receptor-positive breast cancers. Understanding which tumors are associated with RAD51C/D and HRD is key to identify patients who can benefit from targeted therapies, such as PARP (poly [adenosine diphosphate-ribose] polymerase) inhibitors.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
