

Rheumatoid arthritis and idiopathic pulmonary fibrosis: a bidirectional Mendelian randomisation study
- PMID: 38649271
- PMCID: PMC11137470
- DOI: 10.1136/thorax-2023-220856
Rheumatoid arthritis and idiopathic pulmonary fibrosis: a bidirectional Mendelian randomisation study
Abstract
Background: A usual interstitial pneumonia (UIP) pattern of lung injury is a key feature of idiopathic pulmonary fibrosis (IPF) and is also observed in up to 40% of individuals with rheumatoid arthritis (RA)-associated interstitial lung disease (RA-ILD). The RA-UIP phenotype could result from either a causal relationship of RA on UIP or vice versa, or from a simple co-occurrence of RA and IPF due to shared demographic, genetic or environmental risk factors.
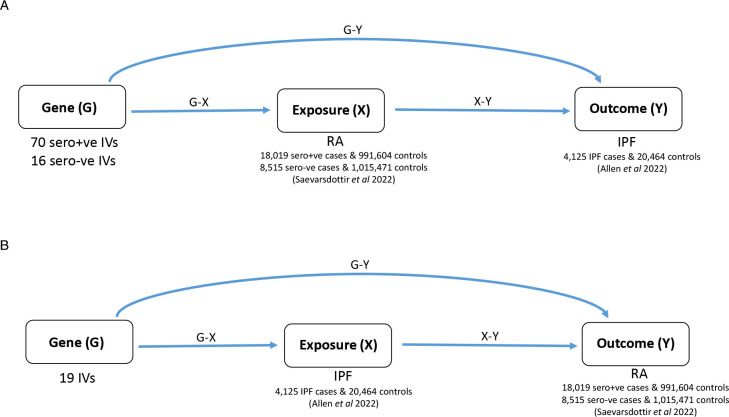
Methods: We used two-sample bidirectional Mendelian randomisation (MR) to test the hypothesis of a causal effect of RA on UIP and of UIP on RA, using variants from genome-wide association studies (GWAS) of RA (separately for seropositive (18 019 cases and 991 604 controls) and seronegative (8515 cases and 1 015 471 controls) RA) and of IPF (4125 cases and 20 464 controls) as genetic instruments. Sensitivity analyses were conducted to assess the robustness of the results to violations of the MR assumptions.
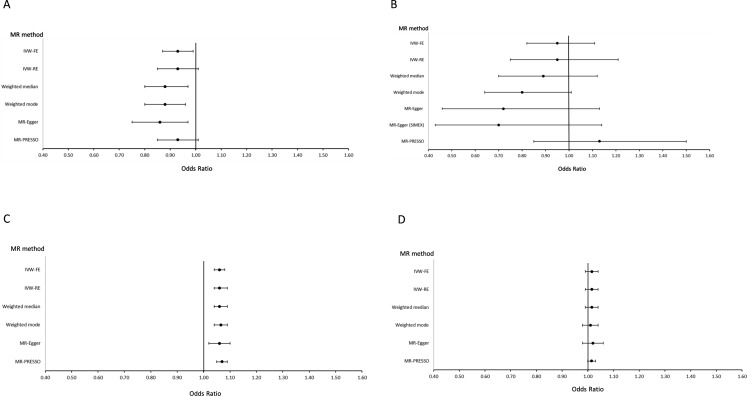
Findings: IPF showed a significant causal effect on seropositive RA, with developing IPF increasing the risk of seropositive RA (OR=1.06, 95% CI: 1.04 to 1.08, p<0.001) which was robust under all models. For the MR in the other direction, seropositive RA showed a significant protective effect on IPF (OR=0.93; 95% CI: 0.87 to 0.99; p=0.032), but the effect was not significant when sensitivity analyses were applied. This was likely because of bias due to exclusion of patients with RA from among the cases in the IPF GWAS, or possibly because our genetic instruments did not fully capture the effect of the complex human leucocyte antigen region, the strongest RA genetic risk factor.
Interpretation: Our findings support the hypothesis that RA-UIP may be due to a cause-effect relationship between UIP and RA, rather than due to a coincidental occurrence of IPF in patients with RA. The significant causal effect of IPF on seropositive RA suggests that pathomechanisms involved in the development of UIP may promote RA, and this may help inform future guidelines on screening for ILD in patients with RA.
Keywords: Idiopathic pulmonary fibrosis; Interstitial Fibrosis; Rheumatoid lung disease.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: LK-D reports funding from Bristol Myers Squibb and Boehringer Ingelheim, outside the submitted work. JKQ reports funding from MRC, HDR UK, GlaxoSmithKline, Bayer, Boehringer Ingelheim, asthma+lung, Chiesi and AstraZeneca; and consultancy fees from GlaxoSmithKline, Boehringer Ingelheim, AstraZeneca, Chiesi, Teva, Insmed and Bayer, outside the submitted work. LVW reports funding from GSK, Pfizer, Orion Pharma, Nordic Bioscience, AstraZeneca, Sysmex and Genentech, outside the submitted work. LVW reports consultancy for Galapagos and Boehringer Ingelheim. RB reports funding from Roche and Boehringer Ingelheim and personal fees for meeting attendance/travel, speaking fees or consulting fees from Sanofi, Roche, Ferrer and Boehringer Ingelheim, outside the submitted work. PD reports funding from Bristol Myers Squibb, Pfizer, Galapagos and Chugai and personal fees for advisory board participation, speaking fees or consulting fees from Boehringer Ingelheim, Bristol Myers Squibb, Janssen, AbbVie, Pfizer, Novartis and Galapagos, outside the submitted work. JKQ reports funding from MRC, HDR UK, GlaxoSmithKline, Bayer, Boehringer Ingelheim, asthma+lung, Chiesi and AstraZeneca; and consultancy fees from GlaxoSmithKline, Boehringer Ingelheim, AstraZeneca, Chiesi, Teva, Insmed and Bayer, outside the submitted work. GJ reports funding from AstraZeneca, Biogen, Galecto, GlaxoSmithKline, Nordic Biosciences, RedX and Pliant, outside this submitted work. GJ reports consultancy for AstraZeneca, Brainomix, Bristol Myers Squibb, Chiesi, Cohbar, Daewoong, GlaxoSmithKline, Veracyte, Resolution Therapeutics and Pilant; and is the president of Action for Pulmonary Fibrosis.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical