

Differentially co-expressed myofibre transcripts associated with abnormal myofibre proportion in chronic obstructive pulmonary disease
- PMID: 38649783
- PMCID: PMC11154789
- DOI: 10.1002/jcsm.13473
Differentially co-expressed myofibre transcripts associated with abnormal myofibre proportion in chronic obstructive pulmonary disease
Abstract
Background: Skeletal muscle dysfunction is a common extrapulmonary manifestation of chronic obstructive pulmonary disease (COPD). Alterations in skeletal muscle myosin heavy chain expression, with reduced type I and increased type II myosin heavy chain expression, are associated with COPD severity when studied in largely male cohorts. The objectives of this study were (1) to define an abnormal myofibre proportion phenotype in both males and females with COPD and (2) to identify transcripts and transcriptional networks associated with abnormal myofibre proportion in COPD.
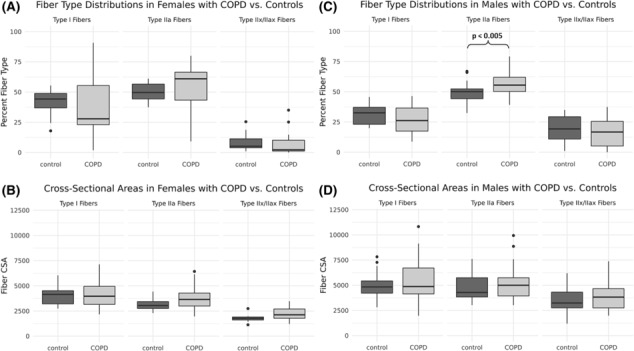
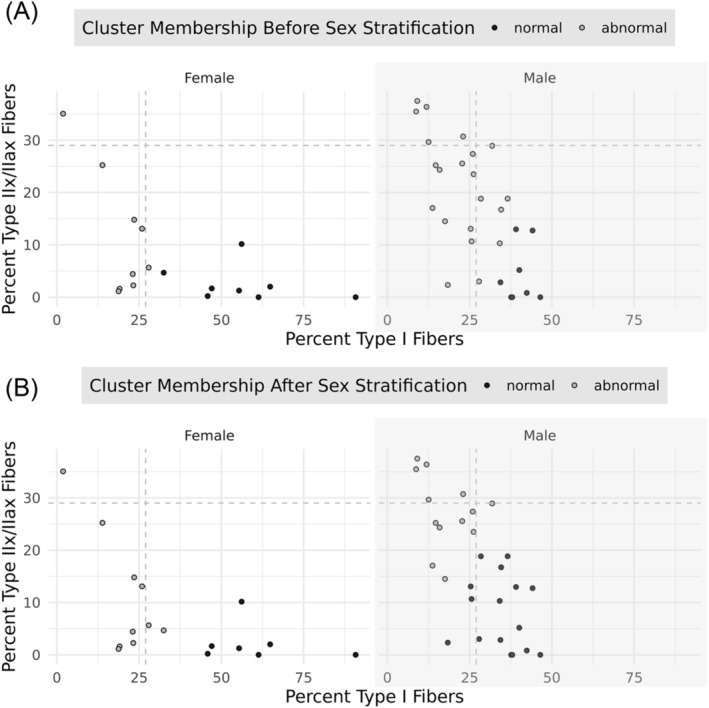
Methods: Forty-six participants with COPD were assessed for body composition, strength, endurance and pulmonary function. Skeletal muscle biopsies from the vastus lateralis were assayed for fibre-type distribution and cross-sectional area via immunofluorescence microscopy and RNA-sequenced to generate transcriptome-wide gene expression data. Sex-stratified k-means clustering of type I and IIx/IIax fibre proportions was used to define abnormal myofibre proportion in participants with COPD and contrasted with previously defined criteria. Single transcripts and weighted co-expression network analysis modules were tested for correlation with the abnormal myofibre proportion phenotype.
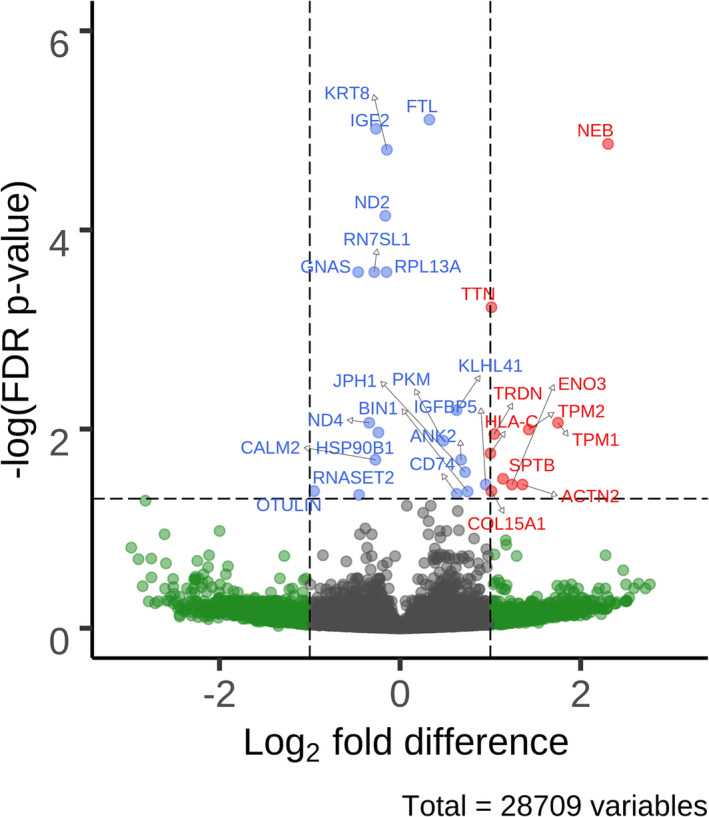
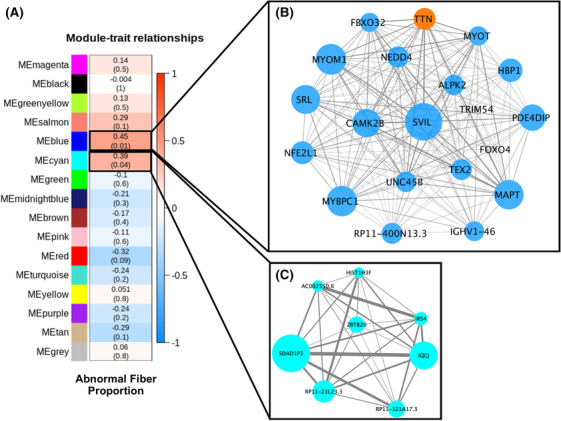
Results: Abnormal myofibre proportion was defined in males with COPD (n = 29) as <18% type I and/or >22% type IIx/IIax fibres and in females with COPD (n = 17) as <36% type I and/or >12% type IIx/IIax fibres. Half of the participants with COPD were classified as having an abnormal myofibre proportion. Participants with COPD and an abnormal myofibre proportion had lower median handgrip strength (26.1 vs. 34.0 kg, P = 0.022), 6-min walk distance (300 vs. 353 m, P = 0.039) and forced expiratory volume in 1 s-to-forced vital capacity ratio (0.42 vs. 0.48, P = 0.041) compared with participants with COPD and normal myofibre proportions. Twenty-nine transcripts were associated with abnormal myofibre proportions in participants with COPD, with the upregulated NEB, TPM1 and TPM2 genes having the largest fold differences. Co-expression network analysis revealed that two transcript modules were significantly positively associated with the presence of abnormal myofibre proportions. One of these co-expression modules contained genes classically associated with muscle atrophy, as well as transcripts associated with both type I and type II myofibres, and was enriched for genetic loci associated with bone mineral density.
Conclusions: Our findings indicate that there are significant transcriptional alterations associated with abnormal myofibre proportions in participants with COPD. Transcripts canonically associated with both type I and type IIa fibres were enriched in a co-expression network associated with abnormal myofibre proportion, suggesting altered transcriptional regulation across multiple fibre types.
Keywords: COPD; fibre‐type shift; myofibre proportions; sex differences; skeletal muscle; transcriptomics.
© 2024 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by Wiley Periodicals LLC.
Conflict of interest statement
HBR reports consulting fees from the NIH RECOVER‐ENERGIZE Working Group (1OT2HL156812) and is involved in contracted clinical research with United Therapeutics, Genentech, Regeneron, Respira and Intervene Immune. He is a visiting professor at the University of Leeds, UK. The remaining authors declare that they have no conflicts of interest.
Figures
References
-
- Vogiatzis I, Terzis G, Stratakos G, Cherouveim E, Athanasopoulos D, Spetsioti S, et al. Effect of pulmonary rehabilitation on peripheral muscle fiber remodeling in patients with COPD in GOLD stages II to IV. Chest 2011;140:744–752. - PubMed
-
- Natanek SA, Gosker HR, Slot IG, Marsh GS, Hopkinson NS, Man WD, et al. Heterogeneity of quadriceps muscle phenotype in chronic obstructive pulmonary disease (COPD); implications for stratified medicine? Muscle Nerve 2013;48:488–497. - PubMed
MeSH terms
Grants and funding
- L70 HL165665/HL/NHLBI NIH HHS/United States
- P50HD098593/NH/NIH HHS/United States
- L70HL165665/NH/NIH HHS/United States
- R01DK122767/NH/NIH HHS/United States
- R01 DK122767/DK/NIDDK NIH HHS/United States
- Parker B. Francis Foundation Fellowship
- T32 HL105346/HL/NHLBI NIH HHS/United States
- F31 HL164006/HL/NHLBI NIH HHS/United States
- I01RX000305/U.S. Department of Veterans Affairs
- R01 AG017896/AG/NIA NIH HHS/United States
- K23AR068450/NH/NIH HHS/United States
- R01HL151452/NH/NIH HHS/United States
- R01 HL153460/HL/NHLBI NIH HHS/United States
- R01HL153460/NH/NIH HHS/United States
- R01HL166850/NH/NIH HHS/United States
- I01 RX000305/RX/RRD VA/United States
- R00 HL121087/HL/NHLBI NIH HHS/United States
- R01 HL166850/HL/NHLBI NIH HHS/United States
- Rheumatology Research Foundation
- R01 HL151452/HL/NHLBI NIH HHS/United States
- T32HL105346/NH/NIH HHS/United States
- T31IP1666/Tobacco-Related Disease Research Program
- R00HL121087/NH/NIH HHS/United States
- P50 HD098593/HD/NICHD NIH HHS/United States
- K23 AR068450/AR/NIAMS NIH HHS/United States
- R01AG017896/NH/NIH HHS/United States
- F31HL164006/NH/NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
