

Rapidly improving ARDS differs clinically and biologically from persistent ARDS
- PMID: 38649920
- PMCID: PMC11034037
- DOI: 10.1186/s13054-024-04883-6
Rapidly improving ARDS differs clinically and biologically from persistent ARDS
Abstract
Background: Rapidly improving acute respiratory distress syndrome (RIARDS) is an increasingly appreciated subgroup of ARDS in which hypoxemia improves within 24 h after initiation of mechanical ventilation. Detailed clinical and biological features of RIARDS have not been clearly defined, and it is unknown whether RIARDS is associated with the hypoinflammatory or hyperinflammatory phenotype of ARDS. The purpose of this study was to define the clinical and biological features of RIARDS and its association with inflammatory subphenotypes.
Methods: We analyzed data from 215 patients who met Berlin criteria for ARDS (endotracheally intubated) and were enrolled in a prospective observational cohort conducted at two sites, one tertiary care center and one urban safety net hospital. RIARDS was defined according to previous studies as improvement of hypoxemia defined as (i) PaO2:FiO2 > 300 or (ii) SpO2: FiO2 > 315 on the day following diagnosis of ARDS (day 2) or (iii) unassisted breathing by day 2 and for the next 48 h (defined as absence of endotracheal intubation on day 2 through day 4). Plasma biomarkers were measured on samples collected on the day of study enrollment, and ARDS phenotypes were allocated as previously described.
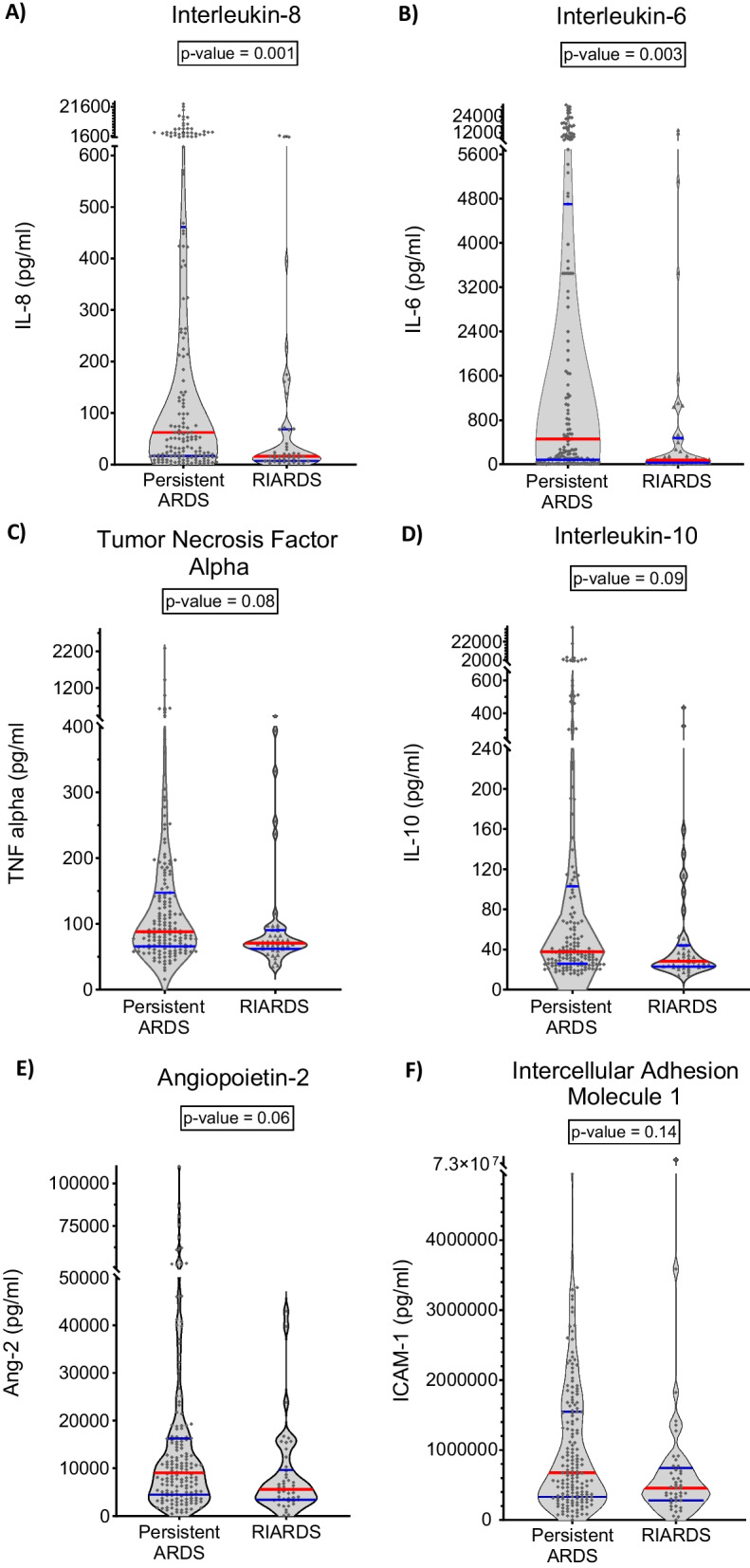
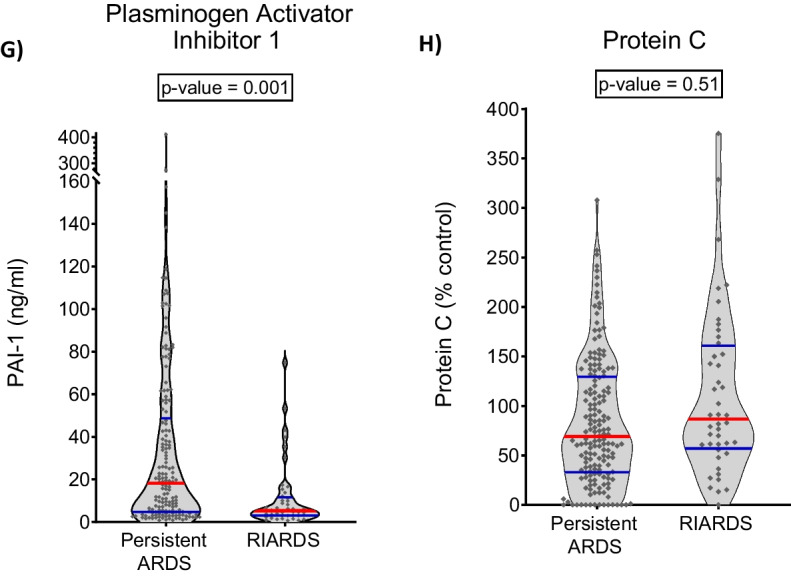
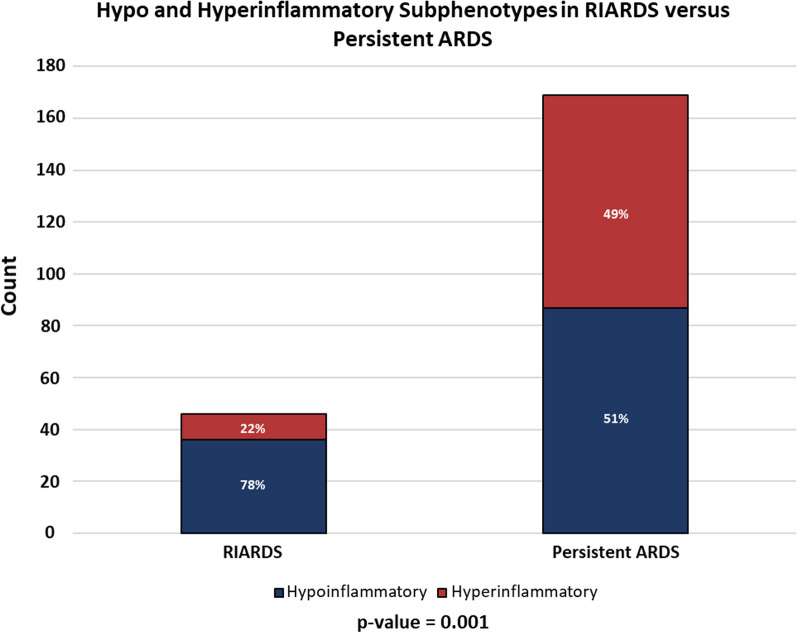
Results: RIARDS accounted for 21% of all ARDS participants. Patients with RIARDS had better clinical outcomes compared to those with persistent ARDS, with lower hospital mortality (13% vs. 57%; p value < 0.001) and more ICU-free days (median 24 vs. 0; p value < 0.001). Plasma levels of interleukin-6, interleukin-8, and plasminogen activator inhibitor-1 were significantly lower among patients with RIARDS. The hypoinflammatory phenotype of ARDS was more common among patients with RIARDS (78% vs. 51% in persistent ARDS; p value = 0.001).
Conclusions: This study identifies a high prevalence of RIARDS in a multicenter observational cohort and confirms the more benign clinical course of these patients. We report the novel finding that RIARDS is characterized by lower concentrations of plasma biomarkers of inflammation compared to persistent ARDS, and that hypoinflammatory ARDS is more prevalent among patients with RIARDS. Identification and exclusion of RIARDS could potentially improve prognostic and predictive enrichment in clinical trials.
Keywords: Acute respiratory distress syndrome; Hypoinflammatory and hyperinflammatory ARDS phenotypes; Precision medicine; Prognostic and predictive enrichment of clinical trials; Rapidly improving acute respiratory distress syndrome.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
