

Photocoagulation or sham laser in addition to conventional anti-VEGF therapy in macular edema associated with TelCaps due to diabetic macular edema or retinal vein occlusion (TalaDME): a study protocol for a multicentric, French, two-group, non-commercial, active-control, observer-masked, non-inferiority, randomized controlled clinical trial
- PMID: 38649937
- PMCID: PMC11034085
- DOI: 10.1186/s13063-024-07994-1
Photocoagulation or sham laser in addition to conventional anti-VEGF therapy in macular edema associated with TelCaps due to diabetic macular edema or retinal vein occlusion (TalaDME): a study protocol for a multicentric, French, two-group, non-commercial, active-control, observer-masked, non-inferiority, randomized controlled clinical trial
Abstract
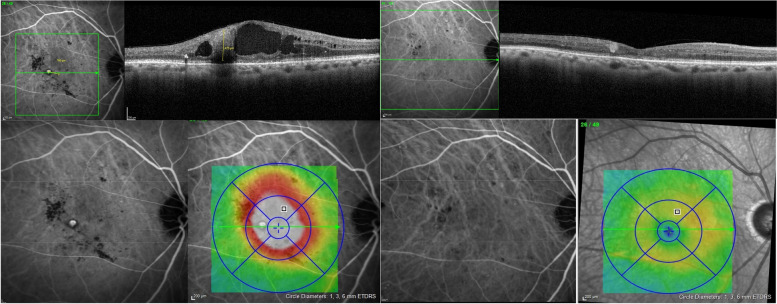
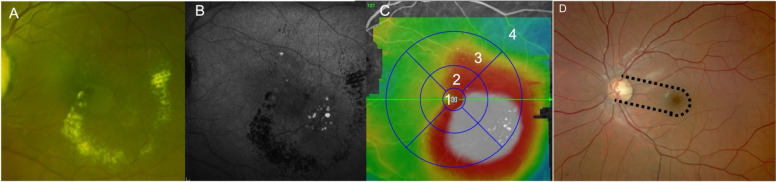
Background: Macular edema (ME) results from hyperpermeability of retinal vessels, leading to chronic extravasation of plasma components into the retina and hence potentially severe visual acuity loss. Current standard of care consists in using intravitreal injections (IVI), which results in a significant medical and economic burden. During diabetic retinopathy (DR) or retinal vein occlusion (RVO), it has recently been shown that focal vascular anomalies (capillary macro-aneurysms, also termed TelCaps) for telangiectatic capillaries may play a central role in the onset, early recurrence, and/or persistence of ME. Since targeted photocoagulation of TelCaps may improve vision, identification, and photocoagulation of TelCaps, it may represent a way to improve management of ME.
Objective: The Targeted Laser in (Diabetic) Macular Edema (TalaDME) study aims to evaluate whether ICG-guided targeted laser (IGTL), in association with standard of care by IVI, allows reducing the number of injections during the first year of treatment compared with IVI only, while remaining non-inferior for visual acuity.
Methods: TalaDME is a French, multicentric, two-arms, randomized, sham laser-controlled, double-masked trial evaluating the effect of photocoagulation of TelCaps combined to IVI in patients with ME associated with TelCaps. Patients with vision loss related to center involved ME secondary to RVO or DR and presenting TelCaps are eligible. Two hundred and seventy eyes of 270 patients are randomized in a 1:1 ratio to standard care, i.e., IVI of anti-VEGF solely (control group) or combined with IGTL therapy (experimental group). Stratification is done on the cause of ME (i.e., RVO versus diabetes). Anti-VEGF IVI are administered to both groups monthly for 3 months (loading dose) and then with a pro re nata regimen with a monthly follow-up for 12 months. The primary endpoint will be the number of IVI and the change in visual acuity from baseline to 12 months. Secondary endpoints will be the changes in central macular thickness, impact on quality of life, cost of treatment, and incremental cost-utility ratio in each groups.
Key safety: Rare but severe AE linked to the use of IVI and laser, and previously described, are expected. In the sham group, rescue laser photocoagulation may be administered by the unmasked investigator if deemed necessary at month 3.
Discussion: The best management of ME associated with TelCaps is debated, and there have been no randomized study designed to answer this question. Given the fact that TelCaps may affect 30 to 60% of patients with chronic ME due to DR or RVO, a large number of patients could benefit from a specific management of TelCaps. TalaDME aims to establish the clinical and medico-economic benefits of additional targeted laser. The results of TalaDME may raise new recommendations for managing ME and impact healthcare costs.
Trial registration: EudraCT: 2018-A00800-55/ NCT03751501. Registration date: Nov. 23, 2018.
Keywords: Diabetic retinopathy; Laser; Macular edema; Photocoagulation; Retinal vein occlusion; Telangiectatic capillaries (TelCaps).
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Photocoagulation for diabetic macular edema. Early treatment diabetic retinopathy study report number 1. Early Treatment Diabetic Retinopathy Study research group. Arch Ophthalmol. 1985;103(12):1796–806. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
