

Comparison between high-flow nasal oxygen (HFNO) alternated with non-invasive ventilation (NIV) and HFNO and NIV alone in patients with COVID-19: a retrospective cohort study
- PMID: 38649940
- PMCID: PMC11036698
- DOI: 10.1186/s40001-024-01826-3
Comparison between high-flow nasal oxygen (HFNO) alternated with non-invasive ventilation (NIV) and HFNO and NIV alone in patients with COVID-19: a retrospective cohort study
Abstract
Background: Non-invasive respiratory support (conventional oxygen therapy [COT], non-invasive ventilation [NIV], high-flow nasal oxygen [HFNO], and NIV alternated with HFNO [NIV + HFNO] may reduce the need for invasive mechanical ventilation (IMV) in patients with COVID-19. The outcome of patients treated non-invasively depends on clinical severity at admission. We assessed the need for IMV according to NIV, HFNO, and NIV + HFNO in patients with COVID-19 according to disease severity and evaluated in-hospital survival rates and hospital and intensive care unit (ICU) lengths of stay.
Methods: This cohort study was conducted using data collected between March 2020 and July 2021. Patients ≥ 18 years admitted to the ICU with a diagnosis of COVID-19 were included. Patients hospitalized for < 3 days, receiving therapy (COT, NIV, HFNO, or NIV + HFNO) for < 48 h, pregnant, and with no primary outcome data were excluded. The COT group was used as reference for multivariate Cox regression model adjustment.
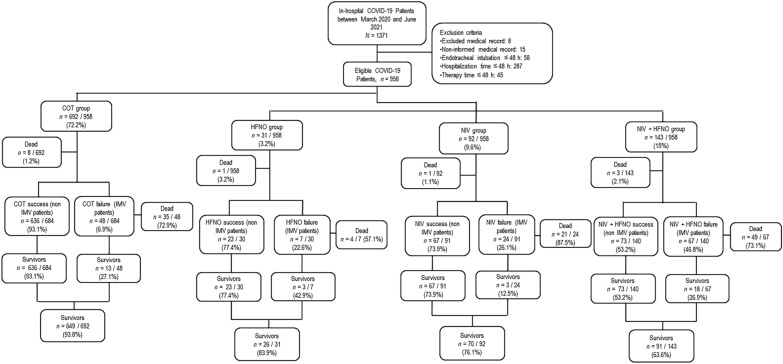
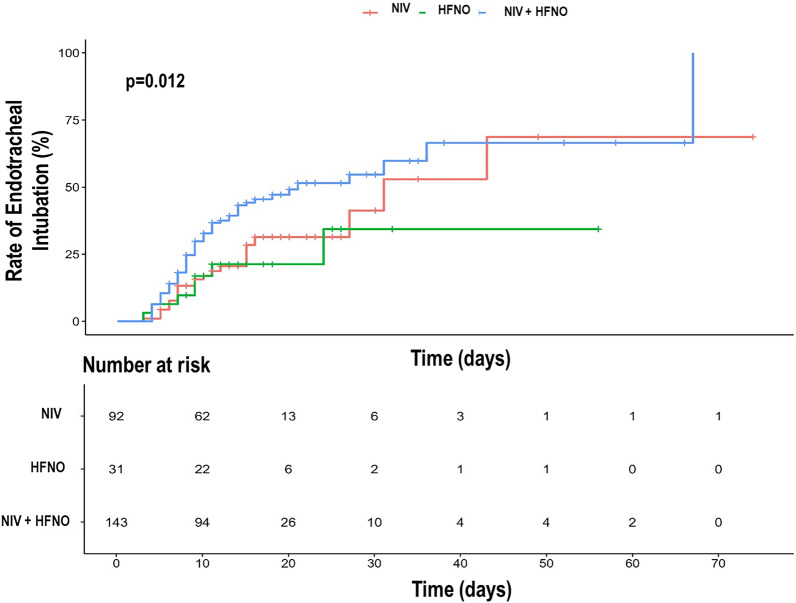
Results: Of 1371 patients screened, 958 were eligible: 692 (72.2%) on COT, 92 (9.6%) on NIV, 31 (3.2%) on HFNO, and 143 (14.9%) on NIV + HFNO. The results for the patients in each group were as follows: median age (interquartile range): NIV (64 [49-79] years), HFNO (62 [55-70] years), NIV + HFNO (62 [48-72] years) (p = 0.615); heart failure: NIV (54.5%), HFNO (36.3%), NIV + HFNO (9%) (p = 0.003); diabetes mellitus: HFNO (17.6%), NIV + HFNO (44.7%) (p = 0.048). > 50% lung damage on chest computed tomography (CT): NIV (13.3%), HFNO (15%), NIV + HFNO (71.6%) (p = 0.038); SpO2/FiO2: NIV (271 [118-365] mmHg), HFNO (317 [254-420] mmHg), NIV + HFNO (229 [102-317] mmHg) (p = 0.001); rate of IMV: NIV (26.1%, p = 0.002), HFNO (22.6%, p = 0.023), NIV + HFNO (46.8%); survival rate: HFNO (83.9%), NIV + HFNO (63.6%) (p = 0.027); ICU length of stay: NIV (8.5 [5-14] days), NIV + HFNO (15 [10-25] days (p < 0.001); hospital length of stay: NIV (13 [10-21] days), NIV + HFNO (20 [15-30] days) (p < 0.001). After adjusting for comorbidities, chest CT score and SpO2/FiO2, the risk of IMV in patients on NIV + HFNO remained high (hazard ratio, 1.88; 95% confidence interval, 1.17-3.04).
Conclusions: In patients with COVID-19, NIV alternating with HFNO was associated with a higher rate of IMV independent of the presence of comorbidities, chest CT score and SpO2/FiO2. Trial registration ClinicalTrials.gov identifier: NCT05579080.
Keywords: COVID-19; High-flow nasal oxygen; Invasive mechanical ventilation; Non-invasive ventilation; Oxygen therapy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Effect of noninvasive ventilation on mortality and clinical outcomes among patients with severe hypoxemic COVID-19 pneumonia after high-flow nasal oxygen failure: a multicenter retrospective French cohort with propensity score analysis.Respir Res. 2024 Jul 15;25(1):279. doi: 10.1186/s12931-024-02873-4. Respir Res. 2024. PMID: 39010097 Free PMC article.
-
High-flow nasal oxygen alone or alternating with non-invasive ventilation in critically ill immunocompromised patients with acute respiratory failure: a randomised controlled trial.Lancet Respir Med. 2022 Jul;10(7):641-649. doi: 10.1016/S2213-2600(22)00096-0. Epub 2022 Mar 21. Lancet Respir Med. 2022. PMID: 35325620 Clinical Trial.
-
High-Flow Nasal Oxygen for Severe Hypoxemia: Oxygenation Response and Outcome in Patients with COVID-19.Am J Respir Crit Care Med. 2022 Feb 15;205(4):431-439. doi: 10.1164/rccm.202109-2163OC. Am J Respir Crit Care Med. 2022. PMID: 34861135 Free PMC article.
-
High-flow nasal oxygen therapy compared with conventional oxygen therapy in hospitalised patients with respiratory illness: a systematic review and meta-analysis.BMJ Open Respir Res. 2024 Jul 15;11(1):e002342. doi: 10.1136/bmjresp-2024-002342. BMJ Open Respir Res. 2024. PMID: 39009460 Free PMC article.
-
Effectiveness and Harms of High-Flow Nasal Oxygen for Acute Respiratory Failure: An Evidence Report for a Clinical Guideline From the American College of Physicians.Ann Intern Med. 2021 Jul;174(7):952-966. doi: 10.7326/M20-4675. Epub 2021 Apr 27. Ann Intern Med. 2021. PMID: 33900793 Free PMC article. Review.
Cited by
-
Non-invasive positive pressure ventilation can reduce perioperative mortality in acute aortic dissection patients with hypoxemia.J Thorac Dis. 2024 Sep 30;16(9):5835-5845. doi: 10.21037/jtd-24-163. Epub 2024 Sep 19. J Thorac Dis. 2024. PMID: 39444862 Free PMC article.
-
Mechanical Ventilator-Associated Pneumonia in the COVID-19 Pandemic Era: A Critical Challenge in the Intensive Care Units.Antibiotics (Basel). 2025 Jan 3;14(1):28. doi: 10.3390/antibiotics14010028. Antibiotics (Basel). 2025. PMID: 39858314 Free PMC article.
-
Characteristics and outcomes in severe and critically ill children with first wave SARS-CoV-2 Omicron infection in Northeast China.Front Cell Infect Microbiol. 2025 Apr 15;15:1495783. doi: 10.3389/fcimb.2025.1495783. eCollection 2025. Front Cell Infect Microbiol. 2025. PMID: 40302919 Free PMC article.
-
Comorbidities and Severe COVID-19 Outcomes: A Retrospective Analysis of Hospitalized Patients in Three Counties in Romania.Microorganisms. 2025 Mar 29;13(4):787. doi: 10.3390/microorganisms13040787. Microorganisms. 2025. PMID: 40284624 Free PMC article.
References
-
- Ferreyro BL, Angriman F, Munshi L, Del Sorbo L, Ferguson ND, Rochwerg B, et al. Association of noninvasive oxygenation strategies with all-cause mortality in adults with acute hypoxemic respiratory failure: a systematic review and meta-analysis. JAMA. 2020;324(1):57–67. doi: 10.1001/jama.2020.9524. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
