

Kinase activities in pancreatic ductal adenocarcinoma with prognostic and therapeutic avenues
- PMID: 38650175
- PMCID: PMC11306541
- DOI: 10.1002/1878-0261.13625
Kinase activities in pancreatic ductal adenocarcinoma with prognostic and therapeutic avenues
Abstract
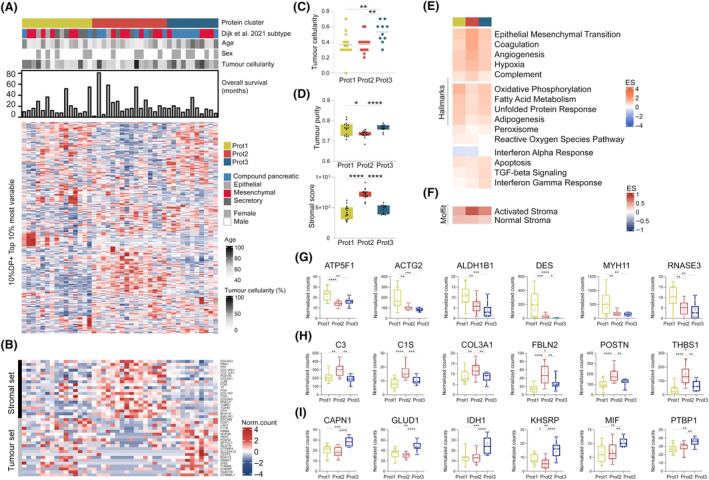
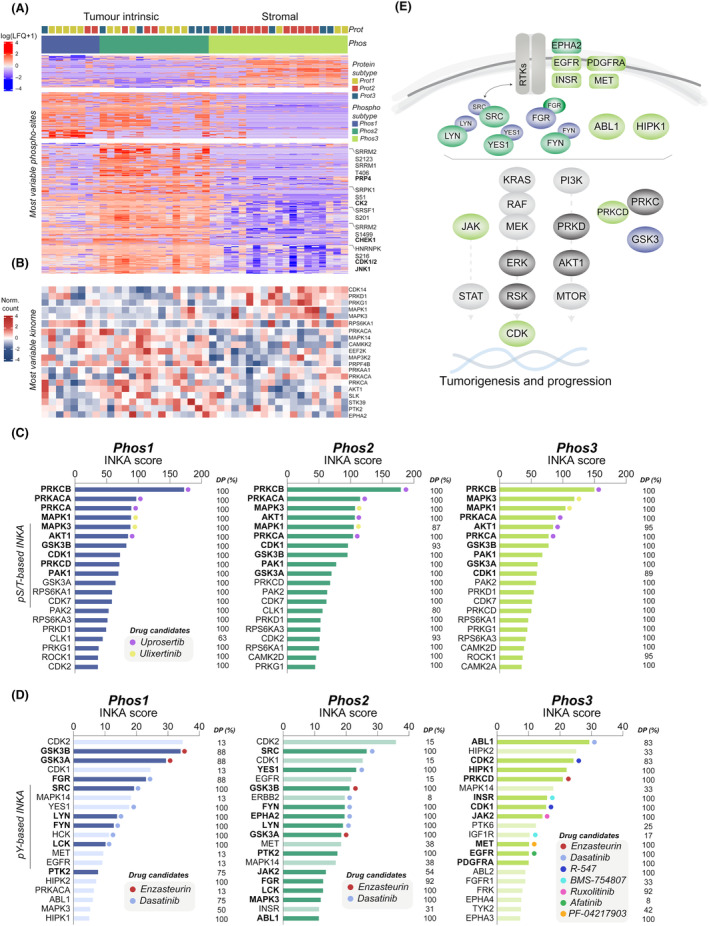
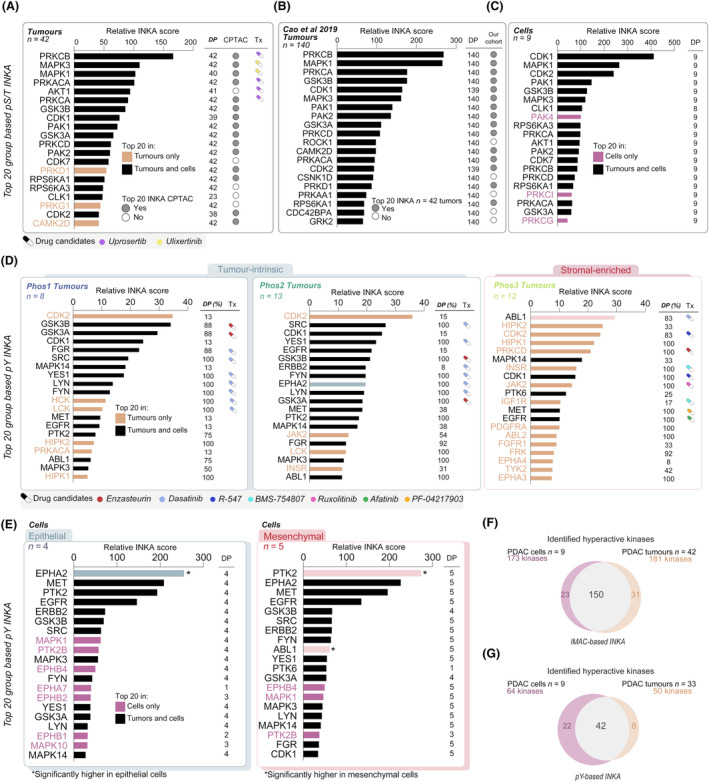
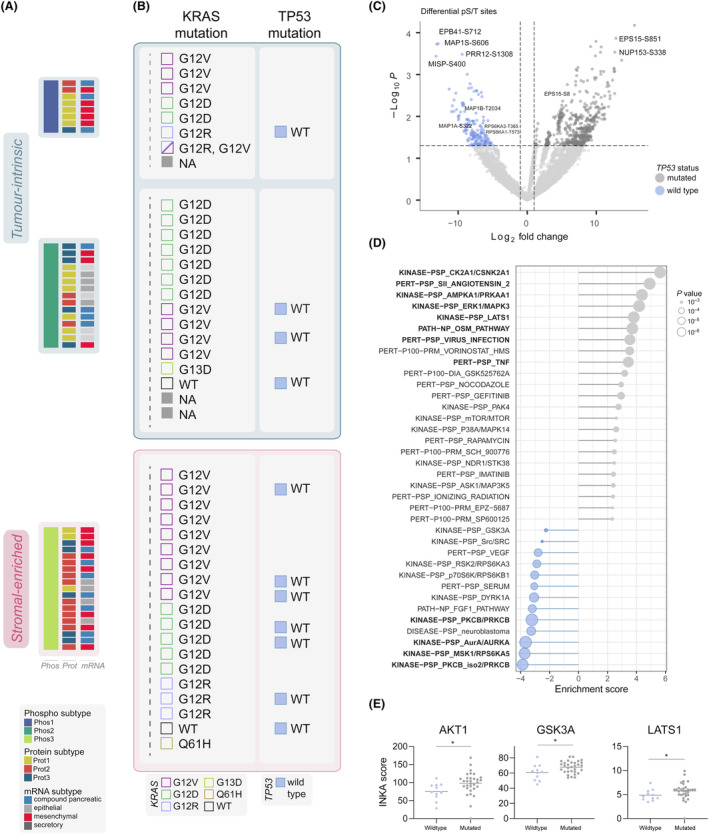
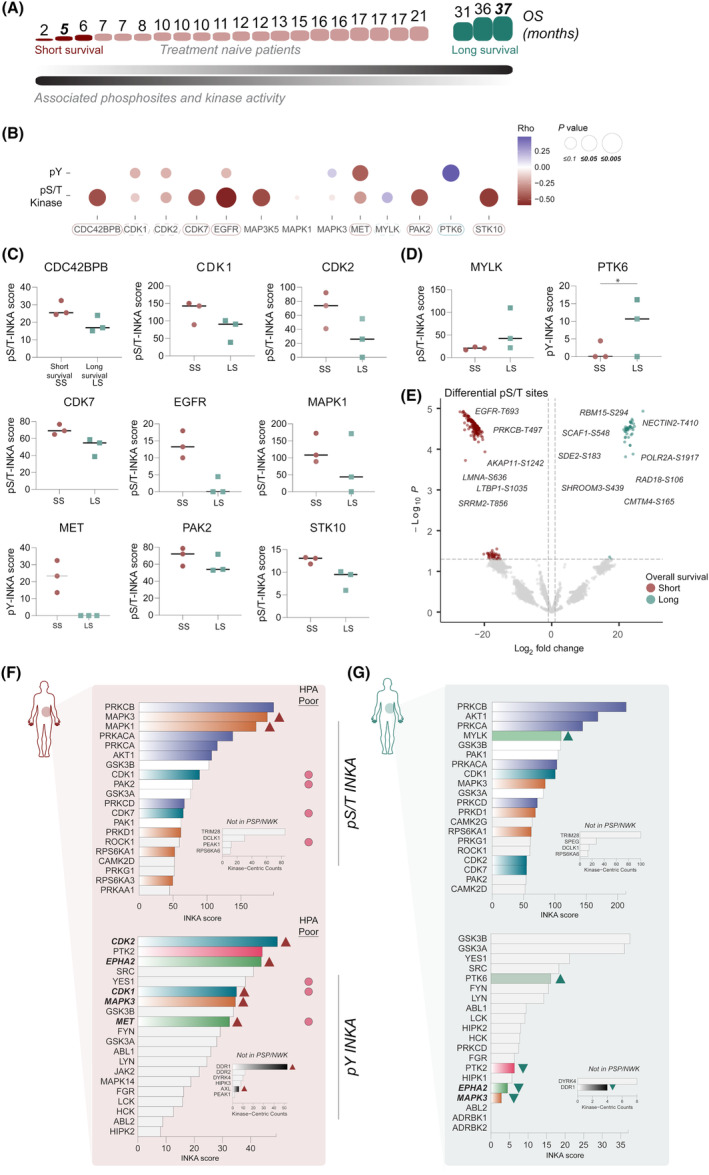
Pancreatic ductal adenocarcinoma (PDAC) is a devastating disease with a limited number of known driver mutations but considerable cancer cell heterogeneity. Phosphoproteomics provides a direct read-out of aberrant signaling and the resultant clinically relevant phenotype. Mass spectrometry (MS)-based proteomics and phosphoproteomics were applied to 42 PDAC tumors. Data encompassed over 19 936 phosphoserine or phosphothreonine (pS/T; in 5412 phosphoproteins) and 1208 phosphotyrosine (pY; in 501 phosphoproteins) sites and a total of 3756 proteins. Proteome data identified three distinct subtypes with tumor intrinsic and stromal features. Subsequently, three phospho-subtypes were apparent: two tumor intrinsic (Phos1/2) and one stromal (Phos3), resembling known PDAC molecular subtypes. Kinase activity was analyzed by the Integrative iNferred Kinase Activity (INKA) scoring. Phospho-subtypes displayed differential phosphorylation signals and kinase activity, such as FGR and GSK3 activation in Phos1, SRC kinase family and EPHA2 in Phos2, and EGFR, INSR, MET, ABL1, HIPK1, JAK, and PRKCD in Phos3. Kinase activity analysis of an external PDAC cohort supported our findings and underscored the importance of PI3K/AKT and ERK pathways, among others. Interestingly, unfavorable patient prognosis correlated with higher RTK, PAK2, STK10, and CDK7 activity and high proliferation, whereas long survival was associated with MYLK and PTK6 activity, which was previously unknown. Subtype-associated activity profiles can guide therapeutic combination approaches in tumor and stroma-enriched tissues, and emphasize the critical role of parallel signaling pathways. In addition, kinase activity profiling identifies potential disease markers with prognostic significance.
Keywords: kinase activity; pancreatic ductal adenocarcinoma; personalized medicine; phosphoproteome.
© 2024 The Authors. Molecular Oncology published by John Wiley & Sons Ltd on behalf of Federation of European Biochemical Societies.
Conflict of interest statement
MFB has received research funding from Celgene, Frame Therapeutics, and Lead Pharma. He has acted as a consultant to Servier. None of these were involved in the design of the study or the drafting of this manuscript.
Figures
Similar articles
-
Phosphoproteomics guides effective low-dose drug combinations against pancreatic ductal adenocarcinoma.Cell Rep. 2023 Jun 27;42(6):112581. doi: 10.1016/j.celrep.2023.112581. Epub 2023 Jun 2. Cell Rep. 2023. PMID: 37269289
-
Resolution of Novel Pancreatic Ductal Adenocarcinoma Subtypes by Global Phosphotyrosine Profiling.Mol Cell Proteomics. 2016 Aug;15(8):2671-85. doi: 10.1074/mcp.M116.058313. Epub 2016 Jun 3. Mol Cell Proteomics. 2016. PMID: 27259358 Free PMC article.
-
The Proteomic Landscape of Pancreatic Ductal Adenocarcinoma Liver Metastases Identifies Molecular Subtypes and Associations with Clinical Response.Clin Cancer Res. 2020 Mar 1;26(5):1065-1076. doi: 10.1158/1078-0432.CCR-19-1496. Epub 2019 Dec 17. Clin Cancer Res. 2020. PMID: 31848187 Free PMC article.
-
Gene expression profiling of 1200 pancreatic ductal adenocarcinoma reveals novel subtypes.BMC Cancer. 2018 May 29;18(1):603. doi: 10.1186/s12885-018-4546-8. BMC Cancer. 2018. PMID: 29843660 Free PMC article.
-
Therapeutic trends in pancreatic ductal adenocarcinoma (PDAC).Expert Opin Investig Drugs. 2019 Feb;28(2):161-177. doi: 10.1080/13543784.2019.1557145. Epub 2018 Dec 16. Expert Opin Investig Drugs. 2019. PMID: 30539678 Review.
References
-
- Mizrahi JD, Surana R, Valle JW, Shroff RT. Pancreatic cancer. Lancet. 2020;395:2008–2020. - PubMed
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74(11):2913–2921. - PubMed
-
- Strobel O, Lorenz P, Hinz U, Gaida M, König AK, Hank T, et al. Actual five‐year survival after upfront resection for pancreatic ductal adenocarcinoma: who beats the odds? Ann Surg. 2022;275(5):962–971. - PubMed
-
- Springfeld C, Ferrone CR, Katz MHG, Philip PA, Hong TS, Hackert T, et al. Neoadjuvant therapy for pancreatic cancer. Nat Rev Clin Oncol. 2023;20(5):318–337. - PubMed
-
- Collisson EA, Bailey P, Chang DK, Biankin AV. Molecular subtypes of pancreatic cancer. Nat Rev Gastroenterol Hepatol. 2019;16(4):207–220. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
