

Mortality burden of pre-treatment weight loss in patients with non-small-cell lung cancer: A systematic literature review and meta-analysis
- PMID: 38650388
- PMCID: PMC11294038
- DOI: 10.1002/jcsm.13477
Mortality burden of pre-treatment weight loss in patients with non-small-cell lung cancer: A systematic literature review and meta-analysis
Abstract
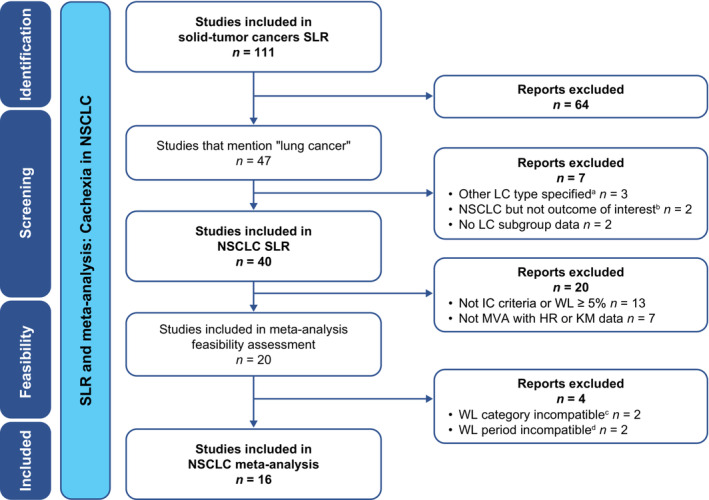
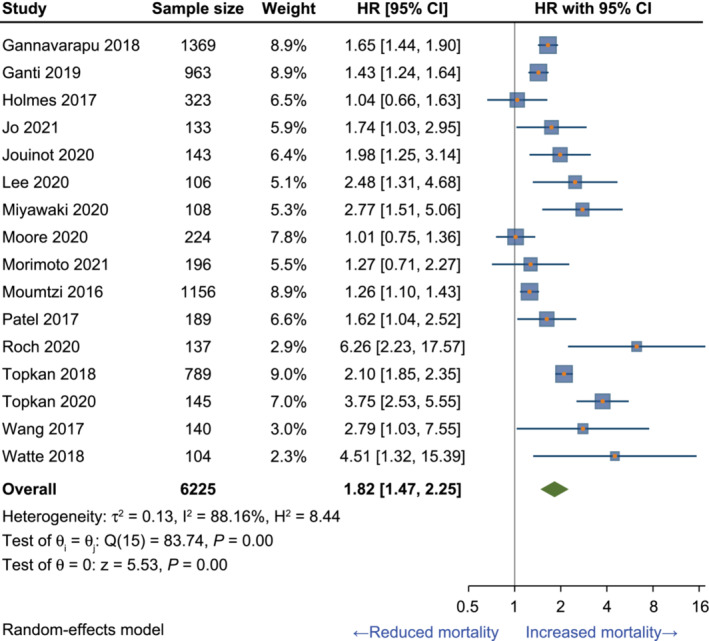
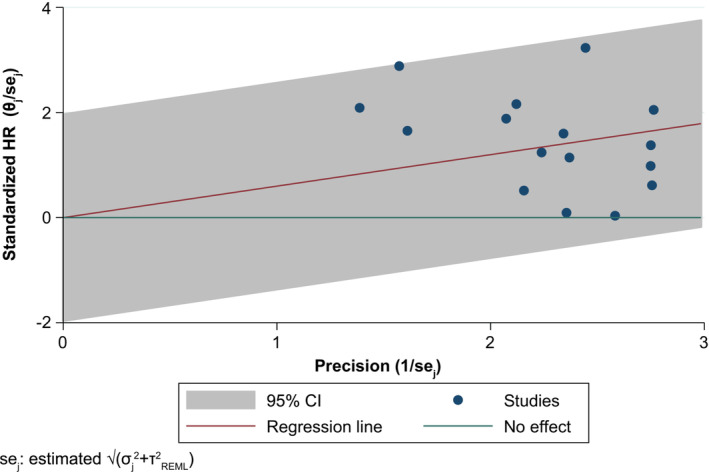
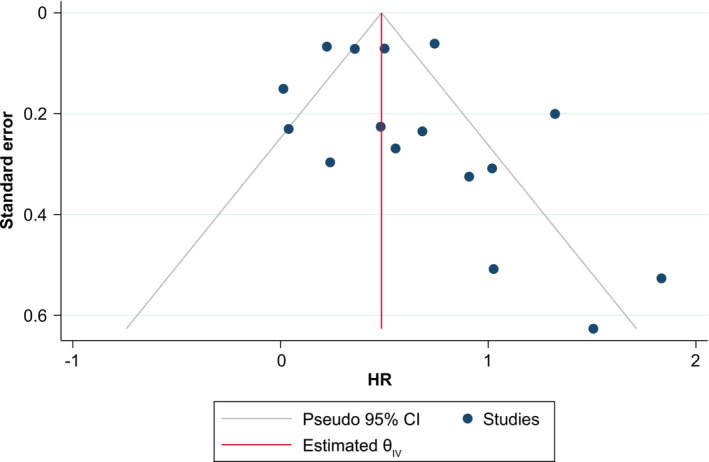
Cachexia, with weight loss (WL) as a major component, is highly prevalent in patients with cancer and indicates a poor prognosis. The primary objective of this study was to conduct a meta-analysis to estimate the risk of mortality associated with cachexia (using established WL criteria prior to treatment initiation) in patients with non-small-cell lung cancer (NSCLC) in studies identified through a systematic literature review. The review was conducted according to PRISMA guidelines. Embase® and PubMed were searched to identify articles on survival outcomes in adult patients with NSCLC (any stage) and cachexia published in English between 1 January 2016 and 10 October 2021. Two independent reviewers screened titles, abstracts and full texts of identified records against predefined inclusion/exclusion criteria. Following a feasibility assessment, a meta-analysis evaluating the impact of cachexia, defined per the international consensus criteria (ICC), or of pre-treatment WL ≥ 5% without a specified time interval, on overall survival in patients with NSCLC was conducted using a random-effects model that included the identified studies as the base case. The impact of heterogeneity was evaluated through sensitivity and subgroup analyses. The standard measures of statistical heterogeneity were calculated. Of the 40 NSCLC publications identified in the review, 20 studies that used the ICC for cachexia or reported WL ≥ 5% and that performed multivariate analyses with hazard ratios (HRs) or Kaplan-Meier curves were included in the feasibility assessment. Of these, 16 studies (80%; n = 6225 patients; published 2016-2021) met the criteria for inclusion in the meta-analysis: 11 studies (69%) used the ICC and 5 studies (31%) used WL ≥ 5%. Combined criteria (ICC plus WL ≥ 5%) were associated with an 82% higher mortality risk versus no cachexia or WL < 5% (pooled HR [95% confidence interval, CI]: 1.82 [1.47, 2.25]). Although statistical heterogeneity was high (I2 = 88%), individual study HRs were directionally aligned with the pooled estimate, and there was considerable overlap in CIs across included studies. A subgroup analysis of studies using the ICC (HR [95% CI]: 2.26 [1.80, 2.83]) or WL ≥ 5% (HR [95% CI]: 1.28 [1.12, 1.46]) showed consistent findings. Assessments of methodological, clinical and statistical heterogeneity indicated that the meta-analysis was robust. Overall, this analysis found that ICC-defined cachexia or WL ≥ 5% was associated with inferior survival in patients with NSCLC. Routine assessment of both weight and weight changes in the oncology clinic may help identify patients with NSCLC at risk for worse survival, better inform clinical decision-making and assess eligibility for cachexia clinical trials.
Keywords: cachexia; meta‐analysis; muscle wasting; non‐small‐cell lung cancer; systematic literature review; weight loss.
© 2024 Pfizer Inc and The Authors. Journal of Cachexia, Sarcopenia and Muscle published by Wiley Periodicals LLC.
Conflict of interest statement
Philip D. Bonomi reports honoraria from Pfizer, Helsinn Healthcare and Roche Genentech. Jeffrey Crawford reports consulting/advisory roles for and honoraria from Actimed Therapeutics, AVEO, Enzychem Lifesciences, Faraday Pharmaceuticals, G1 Therapeutics, Merck, Partner Therapeutics, Pfizer, Sandoz, BIO Alta and Seagen and research funding from Helsinn Healthcare, AstraZeneca and Pfizer (paid to his institution). Richard F. Dunne reports honoraria from Helsinn Healthcare, Exelixis, Toray Industries and Merck. Eric J. Roeland reports participation in scientific advisory boards for Napo Pharmaceuticals, Care4ward, Actimed Therapeutics, Meter Health, Alerion and Takeda; consulting roles for Veloxis Therapeutics and BYOMass; and participation in data safety monitoring boards for Enzychem Lifesciences. Karen E. Smoyer is an employee of Curo, part of the Envision Pharma Group, who were paid consultants to Pfizer in relation to this work. Mohd Kashif Siddiqui is an employee of EBM Health Consultants, who were paid consultants to Envision Pharma Group in relation to this work. Thomas D. McRae and James H. Revkin were employees of Pfizer at the time of the analysis and may hold stock or stock options in Pfizer. Michelle I. Rossulek and Lisa C. Tarasenko are employees of Pfizer and may hold stock or stock options in Pfizer.
Figures
References
-
- Fearon K, Strasser F, Anker SD, Bosaeus I, Bruera E, Fainsinger RL, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol 2011;12:489–495. - PubMed
-
- Bruggeman AR, Kamal AH, LeBlanc TW, Ma JD, Baracos VE, Roeland EJ. Cancer cachexia: beyond weight loss. J Oncol Pract 2016;12:1163–1171. - PubMed
-
- Roeland EJ, Bohlke K, Baracos VE, Bruera E, Del Fabbro E, Dixon S, et al. Management of cancer cachexia: ASCO guideline. J Clin Oncol 2020;38:2438–2453. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
