

Long-term outcomes of intraoperative chemotherapy with 5-FU for colorectal cancer patients receiving curative resection (IOCCRC): a randomized, multicenter, prospective, phase III trial
- PMID: 38652147
- PMCID: PMC11487029
- DOI: 10.1097/JS9.0000000000001301
Long-term outcomes of intraoperative chemotherapy with 5-FU for colorectal cancer patients receiving curative resection (IOCCRC): a randomized, multicenter, prospective, phase III trial
Abstract
Background: The authors aimed to compare combined intraoperative chemotherapy and surgical resection with curative surgical resection alone in colorectal cancer patients.
Methods: The authors performed a multicenter, open-label, randomized, phase III trial. All eligible patients were randomized and assigned to intraoperative chemotherapy and curative surgical resection or curative surgical resection alone (1:1). Survival after long-term follow-up was performed in patients analyzed on an intention-to-treat basis.
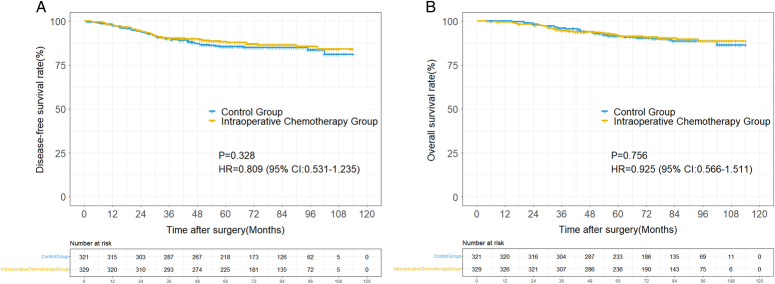
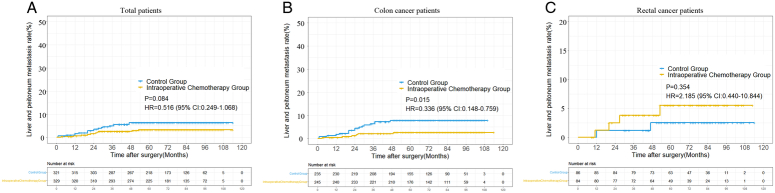
Results: From January 2011 to January 2016, 696 colorectal cancer patients were enrolled and randomly assigned to intraoperative chemotherapy and radical surgical resection ( n =341) or curative surgical resection alone ( n =344). Intraoperative chemotherapy with surgical resection showed no significant survival benefit over surgical resection alone in colorectal cancer patients [3-year disease-free survival (DFS): 91.1 vs. 90.0%, P =0.328; 3-year OS: 94.4 vs. 95.9%, P =0.756). However, colon cancer patients benefitted from intraoperative chemotherapy, with a relative 4% reduction in liver and peritoneal metastasis (HR=0.336, 95% CI: 0.148-0.759, P =0.015) and a 6.5% improvement in 3-year DFS (HR=0.579, 95% CI: 0.353-0.949, P =0.032). Meanwhile, patients with colon cancer and abnormal pretreatment carcinoembryonic antigen (CEA) levels achieved significant survival benefits from intraoperative chemotherapy (DFS: HR=0.464, 95% CI: 0.233-0.921, P =0.029 and OS: HR=0.476, 95% CI: 0.223-1.017, P =0.049).
Conclusions: Intraoperative chemotherapy showed no significant extra prognostic benefit in total colorectal cancer patients who underwent radical surgical resection; however, in colon cancer patients with abnormal pretreatment serum CEA levels (> 5 ng/ml), intraoperative chemotherapy could improve long-term survival.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
All the other authors declare that they have no competing interests.
Figures



References
-
- Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin 2016;66:115–132. - PubMed
-
- André T, Boni C, Mounedji-Boudiaf L, et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med 2004;350:2343–2351. - PubMed
-
- Elferink MA, de Jong KP, Klaase JM, et al. Metachronous metastases from colorectal cancer: a population-based study in North-East Netherlands. Int J Colorectal Dis 2015;30:205–212. - PubMed
-
- Sadahiro S, Suzuki T, Ishikawa K, et al. Recurrence patterns after curative resection of colorectal cancer in patients followed for a minimum of ten years. Hepato-gastroenterology 2003;50:1362–1366. - PubMed
-
- Grothey A. Oxaliplatin-safety profile: neurotoxicity, Seminars in oncology. Elsevier; 2003:5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
