

Serum and Salivary IgG and IgA Response After COVID-19 Messenger RNA Vaccination
- PMID: 38652471
- PMCID: PMC11040412
- DOI: 10.1001/jamanetworkopen.2024.8051
Serum and Salivary IgG and IgA Response After COVID-19 Messenger RNA Vaccination
Abstract
Importance: There is still considerable controversy in the literature regarding the capacity of intramuscular messenger RNA (mRNA) vaccination to induce a mucosal immune response.
Objective: To compare serum and salivary IgG and IgA levels among mRNA-vaccinated individuals with or without previous SARS-CoV-2 infection.
Design, setting, and participants: In this cohort study, SARS-CoV-2-naive participants and those with previous infection were consecutively included in the CoviCompare P and CoviCompare M mRNA vaccination trials and followed up to day 180 after vaccination with either the BNT162b2 (Pfizer-BioNTech) vaccine or the mRNA-1273 (Moderna) vaccine at the beginning of the COVID-19 vaccination campaign (from February 19 to June 8, 2021) in France. Data were analyzed from October 25, 2022, to July 13, 2023.
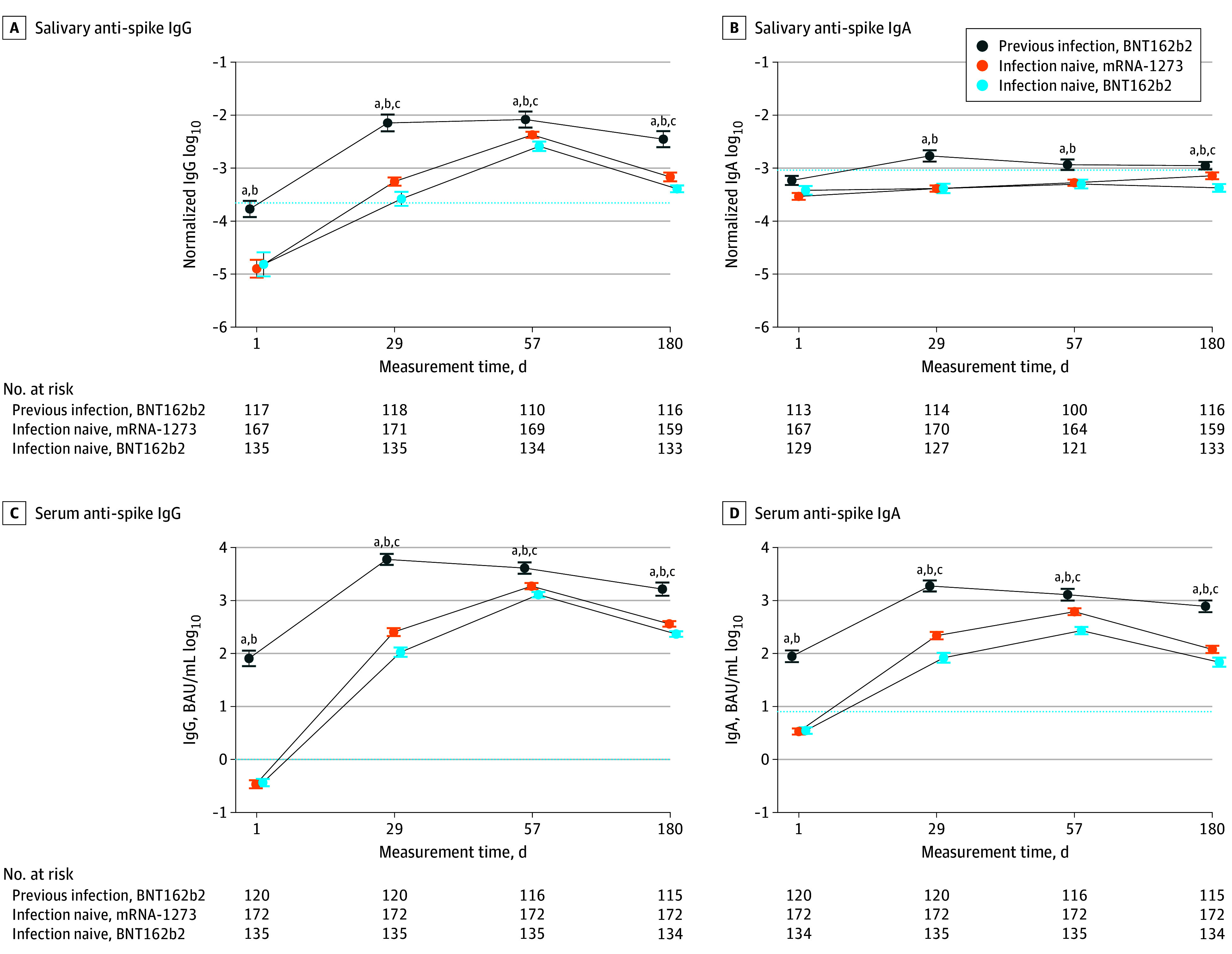
Main outcomes and measures: An ultrasensitive digital enzyme-linked immunosorbent assay was used for the comparison of SARS-CoV-2 spike-specific serum and salivary IgG and IgA levels. Spike-specific secretory IgA level was also quantified at selected times.
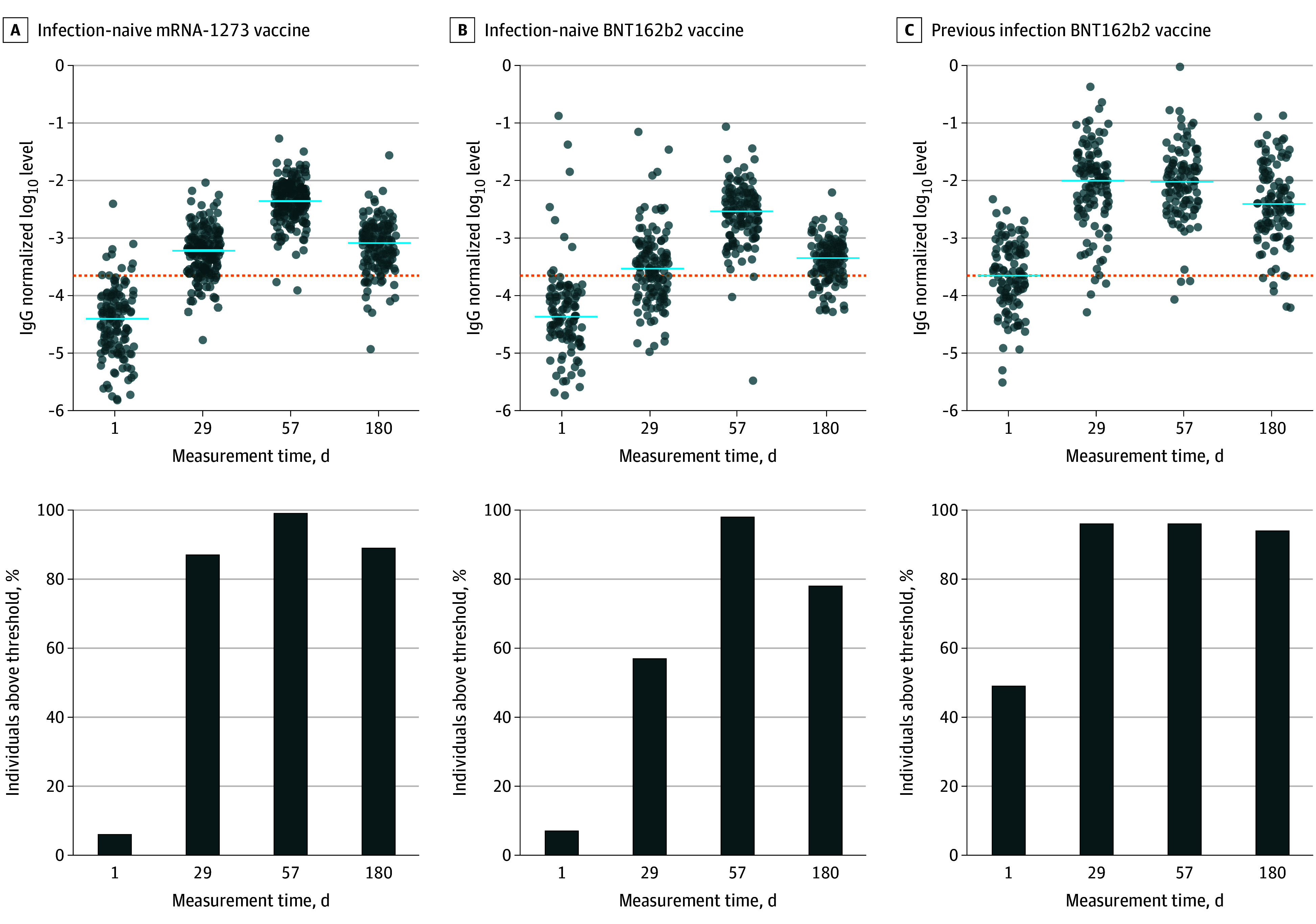
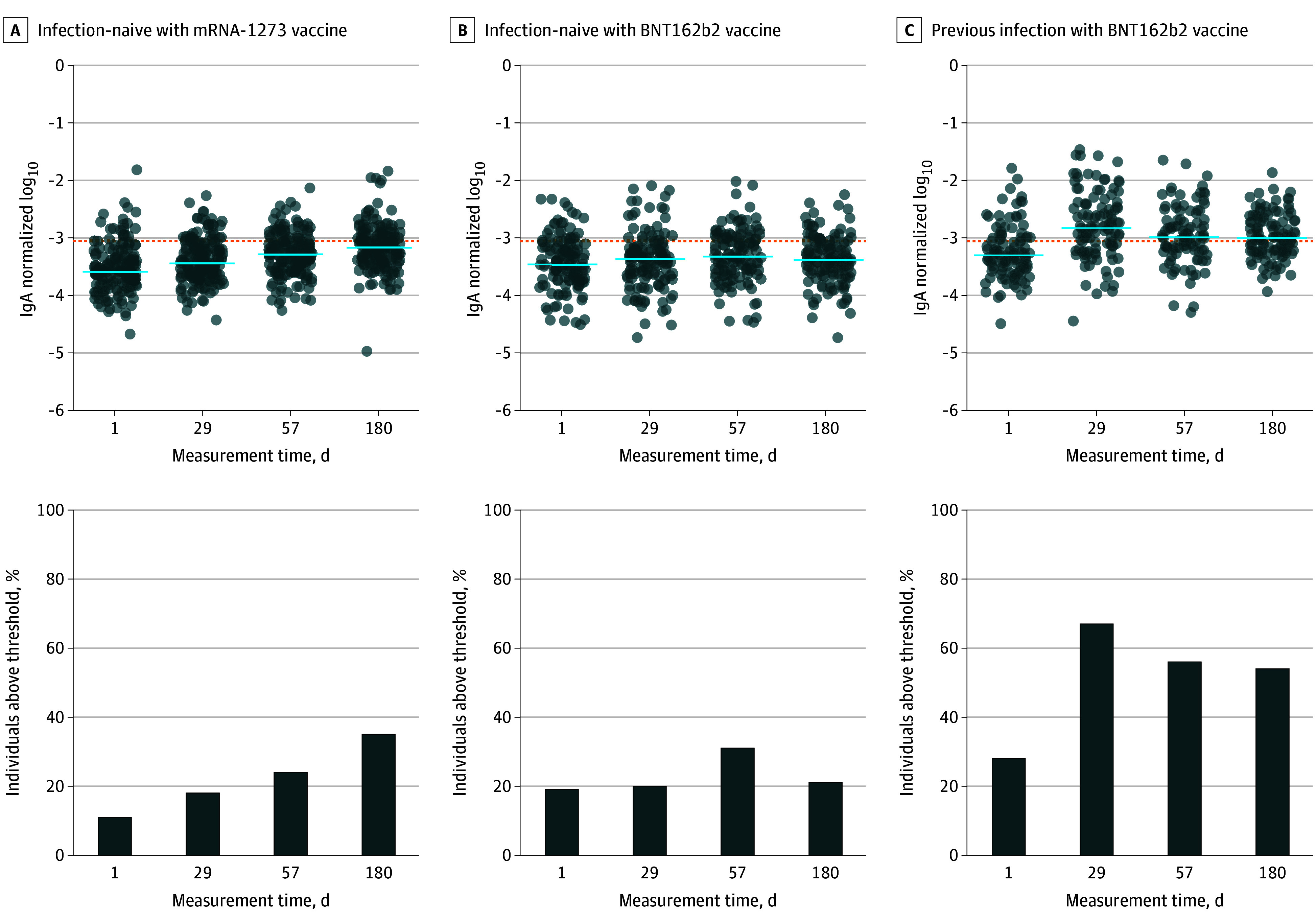
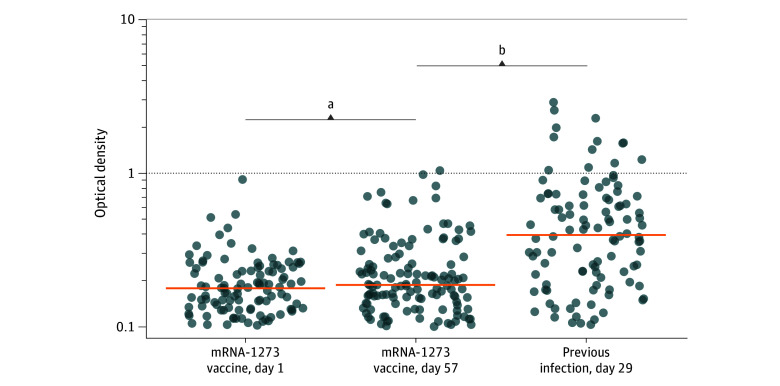
Results: A total of 427 individuals were included in 3 groups: participants with SARS-CoV-2 prior to vaccination who received 1 single dose of BNT162b2 (Pfizer-BioNTech) (n = 120) and SARS-CoV-2-naive individuals who received 2 doses of mRNA-1273 (Moderna) (n = 172) or 2 doses of BNT162b2 (Pfizer-BioNTech) (n = 135). The median age was 68 (IQR, 39-75) years, and 228 (53.4%) were men. SARS-CoV-2 spike-specific IgG saliva levels increased after 1 or 2 vaccine injections in individuals with previous infection and SARS-CoV-2-naive individuals. After vaccination, SARS-CoV-2-specific saliva IgA levels, normalized with respect to total IgA levels, were significantly higher in participants with previous infection, as compared with the most responsive mRNA-1273 (Moderna) recipients (median normalized levels, 155 × 10-5 vs 37 × 10-5 at day 29; 107 × 10-5 vs 54 × 10-5 at day 57; and 104 × 10-5 vs 70 × 10-5 at day 180 [P < .001]). In contrast, compared with day 1, spike-specific IgA levels in the BNT162b2-vaccinated SARS-CoV-2-naive group increased only at day 57 (36 × 10-5 vs 49 × 10-5 [P = .01]). Bona fide multimeric secretory IgA levels were significantly higher in individuals with previous infection compared with SARS-CoV-2-naive individuals after 2 antigenic stimulations (median optical density, 0.36 [IQR, 0.16-0.63] vs 0.16 [IQR, 0.10-0.22]; P < .001).
Conclusions and relevance: The findings of this cohort study suggest that mRNA vaccination was associated with mucosal immunity in individuals without prior SARS-CoV-2 infection, but at much lower levels than in previously infected individuals. Further studies are needed to determine the association between specific saliva IgA levels and prevention of infection or transmission.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
