

Survey of Ventilator Waveform Interpretation Among ICU Professionals
- PMID: 38653558
- PMCID: PMC11285504
- DOI: 10.4187/respcare.11677
Survey of Ventilator Waveform Interpretation Among ICU Professionals
Abstract
Background: The interpretation of ventilator waveforms is essential for effective and safe mechanical ventilation but requires specialized training and expertise. This study aimed to investigate the ability of ICU professionals to interpret ventilator waveforms, identify areas requiring further education and training, and explore the factors influencing their interpretation skills.
Methods: We conducted an international online anonymous survey of ICU professionals (physicians, nurses, and respiratory therapists [RTs]), with ≥ 1 y of experience working in the ICU. The survey consisted of demographic information and 15 multiple-choice questions related to ventilator waveforms. Results were compared between professions using descriptive statistics, and logistic regression (expressed as odds ratios [ORs; 95% CI]) was performed to identify factors associated with high performance, which was defined by a threshold of 60% correct answers.
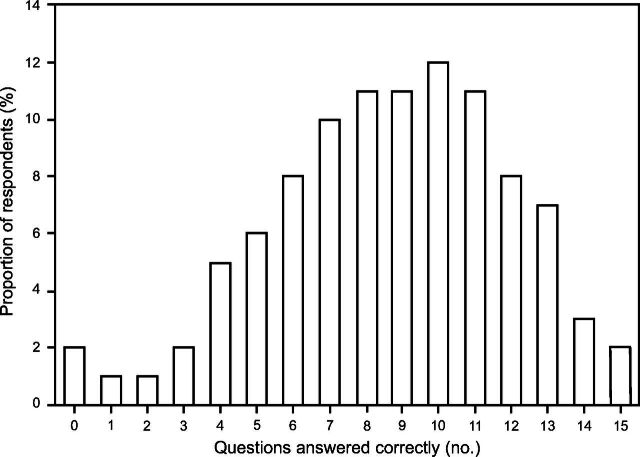
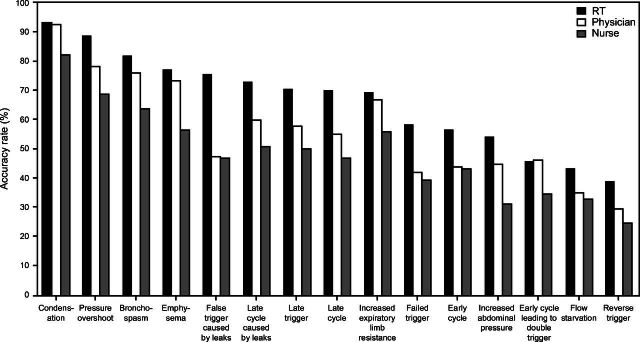
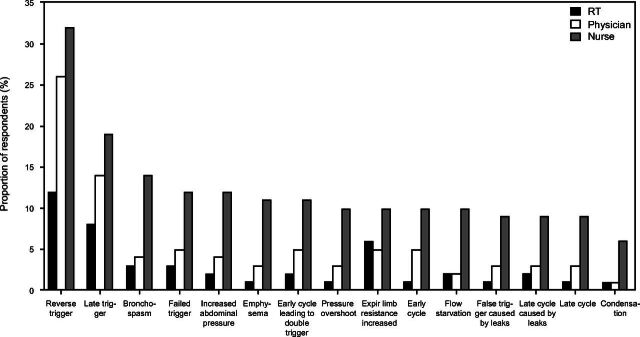
Results: A total of 1,832 professionals from 31 countries or regions completed the survey; 53% of respondents answered ≥ 60% of the questions correctly. The 3 questions with the most correct responses were related to waveforms that demonstrated condensation (90%), pressure overshoot (79%), and bronchospasm (75%). Conversely, the 3 questions with the fewest correct responses were waveforms that demonstrated early cycle leading to double trigger (43%), severe under assistance (flow starvation) (37%), and early/reverse trigger (31%). Factors significantly associated with ≥ 60% correct answers included years of ICU working experience (≥ 10 y, OR 1.6 [1.2-2.0], P < .001), profession (RT, OR 2.8 [2.1-3.7], P < .001), highest degree earned (graduate, OR 1.7 [1.3-2.2], P < .001), workplace (teaching hospital, OR 1.4 [1.1-1.7], P = .008), and prior ventilator waveforms training (OR 1.7 [1.3-2.2], P < .001).
Conclusions: Slightly over half respondents correctly identified ≥ 60% of waveforms demonstrating patient-ventilator discordance. High performance was associated with ≥ 10 years of ICU working experience, RT profession, graduate degree, working in a teaching hospital, and prior ventilator waveforms training. Some discordances were poorly recognized across all groups of surveyed professionals.
Keywords: ICUs; mechanical ventilation; patient-ventilator discordance; ventilator; waveform interpretation.
Copyright © 2024 by Daedalus Enterprises.
Conflict of interest statement
Dr Li discloses relationships with Fisher & Paykel Healthcare, Aerogen, Vincent Medical, the Rice Foundation, the American Association for Respiratory Care, Vincent, and Heyer. Dr Li is a section editor for Respiratory Care. Mr Miller discloses relationships with Saxe Communications, S2N Health, and Fisher & Paykel. Mr Miller is a section editor for Respiratory Care. Dr Mireles-Cabodevila is a co-owner of a patent for mid-frequency ventilation. Dr Mireles-Cabodevila discloses relationships with IngMar Medical and Elsevier. The remaining authors have disclosed no conflicts of interest.
Figures
Similar articles
-
Emergency and critical care medicine residents' competency to identify patient ventilator asynchrony using a mechanical ventilator waveform analysis in Addis Ababa, Ethiopia: a multicenter cross-sectional study.BMC Med Educ. 2025 Feb 4;25(1):180. doi: 10.1186/s12909-025-06748-0. BMC Med Educ. 2025. PMID: 39905426 Free PMC article.
-
Evaluation of health care providers' ability to identify patient-ventilator triggering asynchrony in intensive care unit: a translational observational study in China.BMC Med Educ. 2025 Feb 4;25(1):182. doi: 10.1186/s12909-025-06638-5. BMC Med Educ. 2025. PMID: 39905371 Free PMC article.
-
Factors that impact on the use of mechanical ventilation weaning protocols in critically ill adults and children: a qualitative evidence-synthesis.Cochrane Database Syst Rev. 2016 Oct 4;10(10):CD011812. doi: 10.1002/14651858.CD011812.pub2. Cochrane Database Syst Rev. 2016. PMID: 27699783 Free PMC article.
-
Health professionals' experience of teamwork education in acute hospital settings: a systematic review of qualitative literature.JBI Database System Rev Implement Rep. 2016 Apr;14(4):96-137. doi: 10.11124/JBISRIR-2016-1843. JBI Database System Rev Implement Rep. 2016. PMID: 27532314
-
Oral hygiene care for critically ill patients to prevent ventilator-associated pneumonia.Cochrane Database Syst Rev. 2016 Oct 25;10(10):CD008367. doi: 10.1002/14651858.CD008367.pub3. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2020 Dec 24;12:CD008367. doi: 10.1002/14651858.CD008367.pub4. PMID: 27778318 Free PMC article. Updated.
Cited by
-
Bridging the Gap Between Detection, Understanding, and Future Innovation in Patient-Ventilator Asynchronies.Respir Care. 2024 Jun 28;69(7):902-904. doi: 10.4187/respcare.12153. Respir Care. 2024. PMID: 38942595 Free PMC article. No abstract available.
-
Simulation in Mechanical Ventilation Training: Integrating Best Practices for Effective Education.Respir Care. 2024 Oct 25;69(11):1468-1476. doi: 10.4187/respcare.12551. Respir Care. 2024. PMID: 39455249 No abstract available.
-
Optimizing Mechanical Ventilation: A Clinical and Practical Bedside Method for the Identification and Management of Patient-Ventilator Asynchronies in Critical Care.J Clin Med. 2025 Jan 2;14(1):214. doi: 10.3390/jcm14010214. J Clin Med. 2025. PMID: 39797296 Free PMC article. Review.
References
-
- Mireles-Cabodevila E, Siuba MT, Chatburn RL. A taxonomy for patient-ventilator interactions and a method to read ventilator waveforms. Respir Care 2022;67(1):129-148. - PubMed
-
- Chao DC, Scheinhorn DJ, Stearn-Hassenpflug M. Patient-ventilator trigger asynchrony in prolonged mechanical ventilation. Chest 1997;112(6):1592-1599. - PubMed
-
- Thille AW, Rodriguez P, Cabello B, Lellouche F, Brochard L. Patient-ventilator asynchrony during assisted mechanical ventilation. Intensive Care Med 2006;32(10):1515-1522. - PubMed
-
- Colombo D, Cammarota G, Alemani M, Carenzo L, Barra FL, Vaschetto R, et al. Efficacy of ventilator waveforms observation in detecting patient-ventilator asynchrony. Crit Care Med 2011;39(11):2452-2457. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
