

AI-enabled left atrial volumetry in coronary artery calcium scans (AI-CACTM) predicts atrial fibrillation as early as one year, improves CHARGE-AF, and outperforms NT-proBNP: The multi-ethnic study of atherosclerosis
- PMID: 38653606
- PMCID: PMC11216863
- DOI: 10.1016/j.jcct.2024.04.005
AI-enabled left atrial volumetry in coronary artery calcium scans (AI-CACTM) predicts atrial fibrillation as early as one year, improves CHARGE-AF, and outperforms NT-proBNP: The multi-ethnic study of atherosclerosis
Abstract
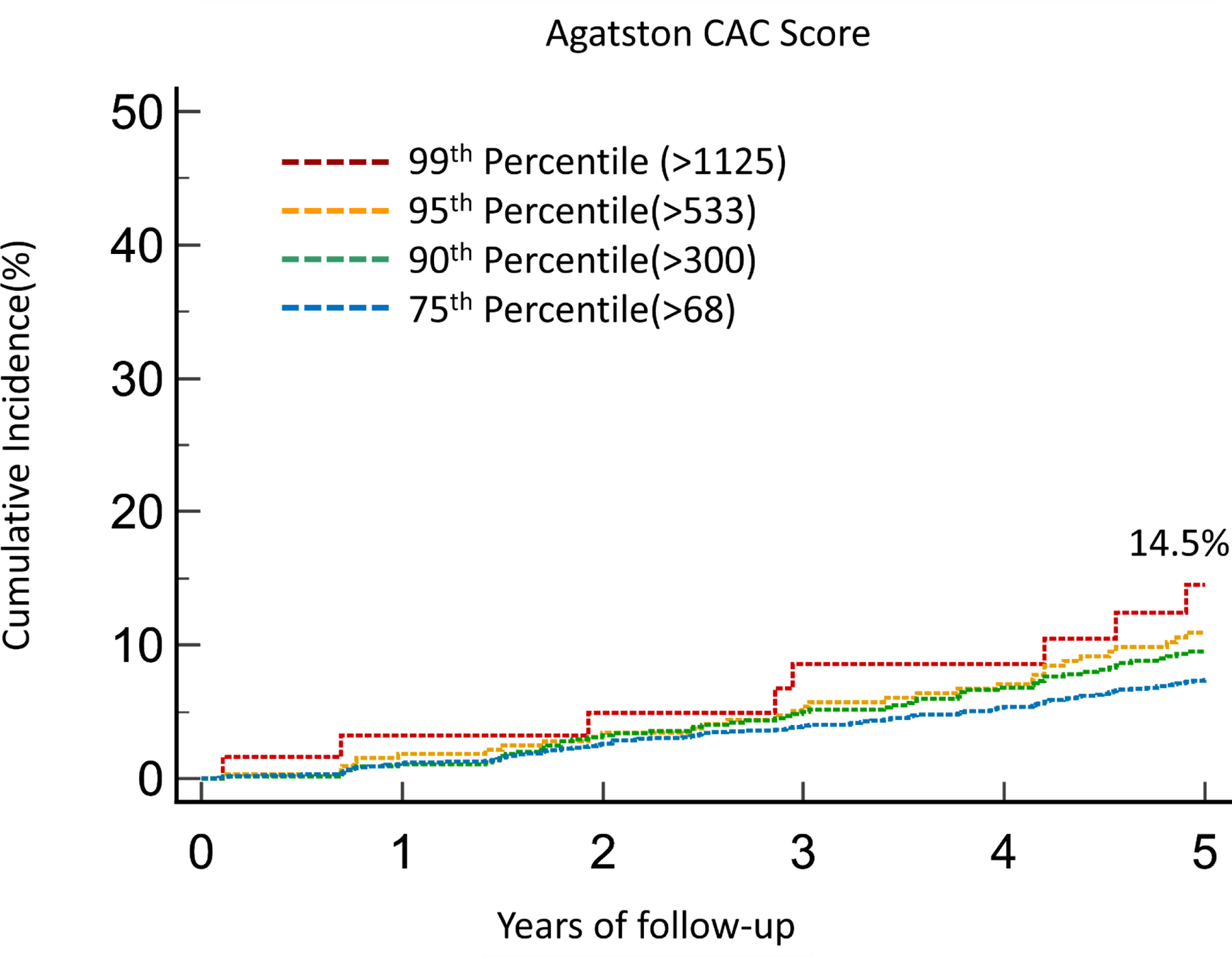
Background: Coronary artery calcium (CAC) scans contain actionable information beyond CAC scores that is not currently reported.
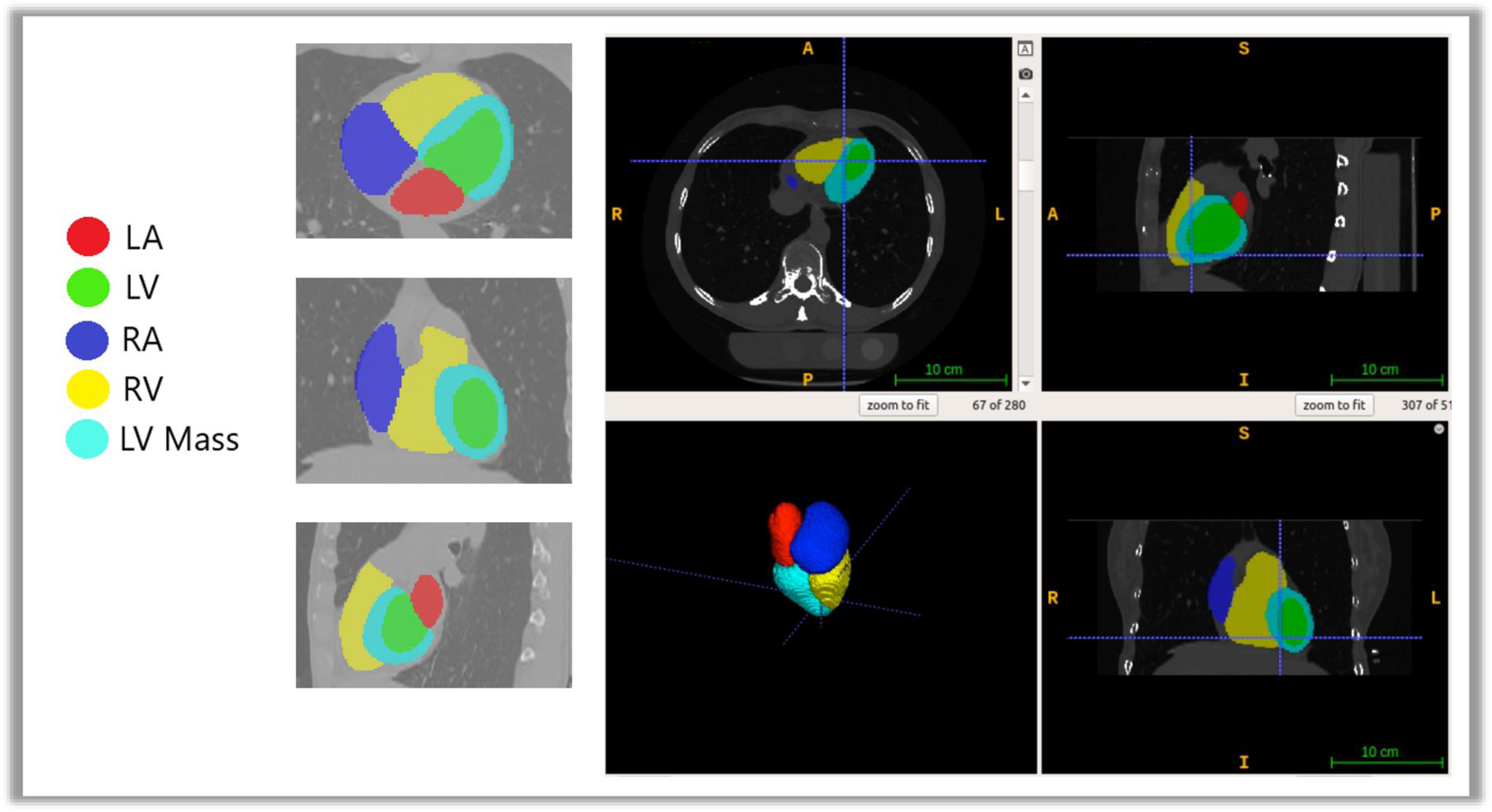
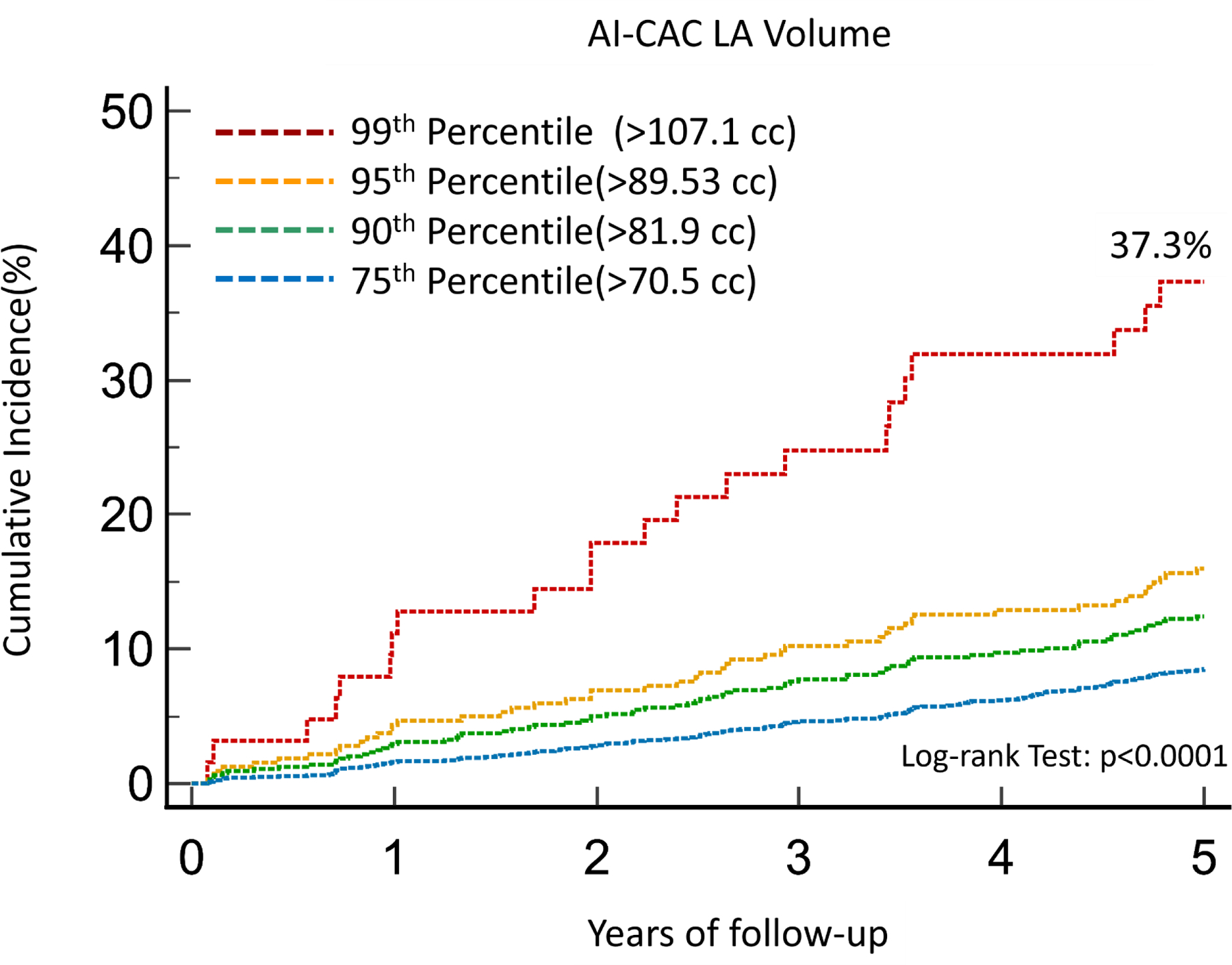
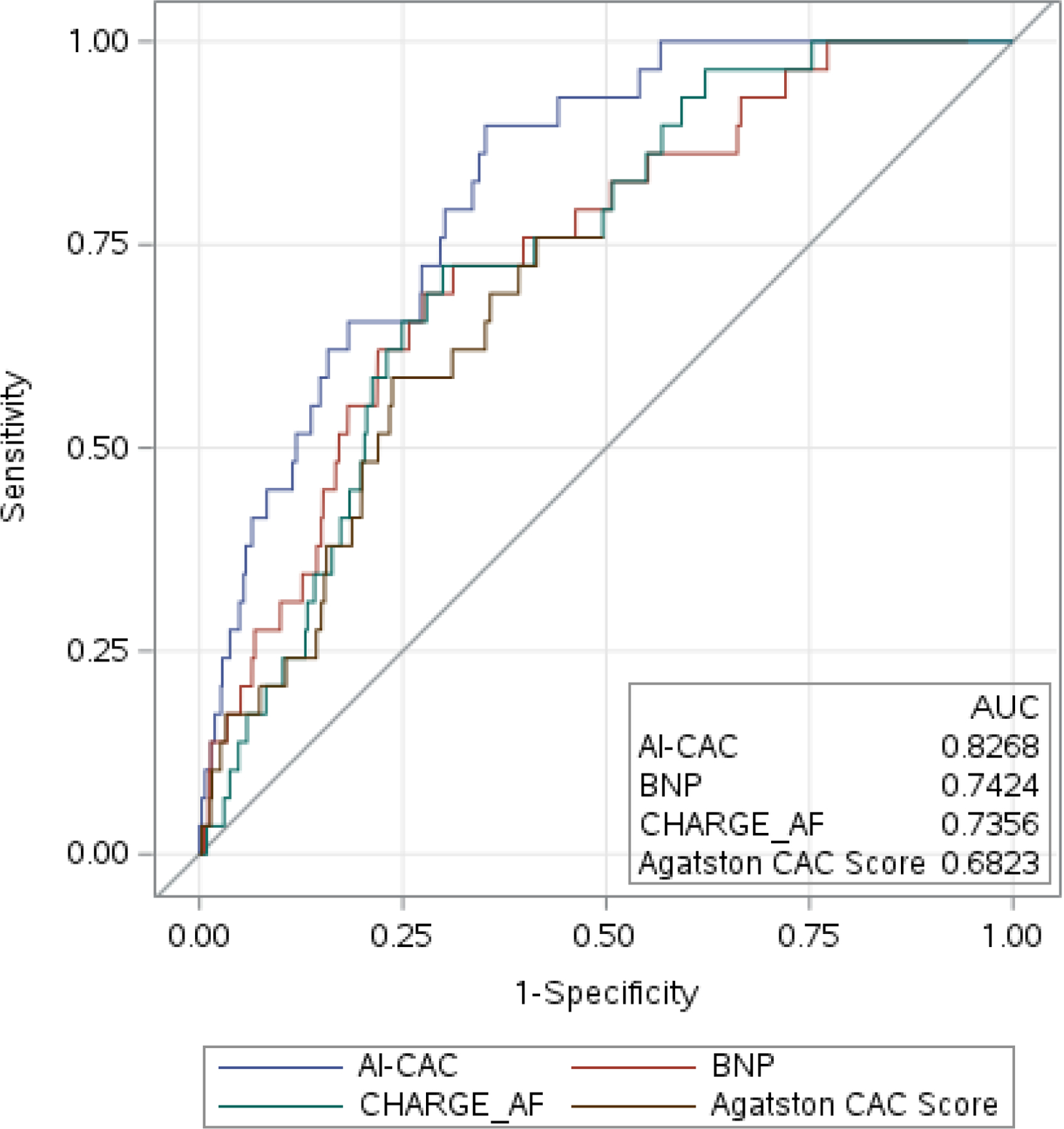
Methods: We have applied artificial intelligence-enabled automated cardiac chambers volumetry to CAC scans (AI-CACTM) to 5535 asymptomatic individuals (52.2% women, ages 45-84) that were previously obtained for CAC scoring in the baseline examination (2000-2002) of the Multi-Ethnic Study of Atherosclerosis (MESA). AI-CAC took on average 21 s per CAC scan. We used the 5-year outcomes data for incident atrial fibrillation (AF) and assessed discrimination using the time-dependent area under the curve (AUC) of AI-CAC LA volume with known predictors of AF, the CHARGE-AF Risk Score and NT-proBNP. The mean follow-up time to an AF event was 2.9 ± 1.4 years.
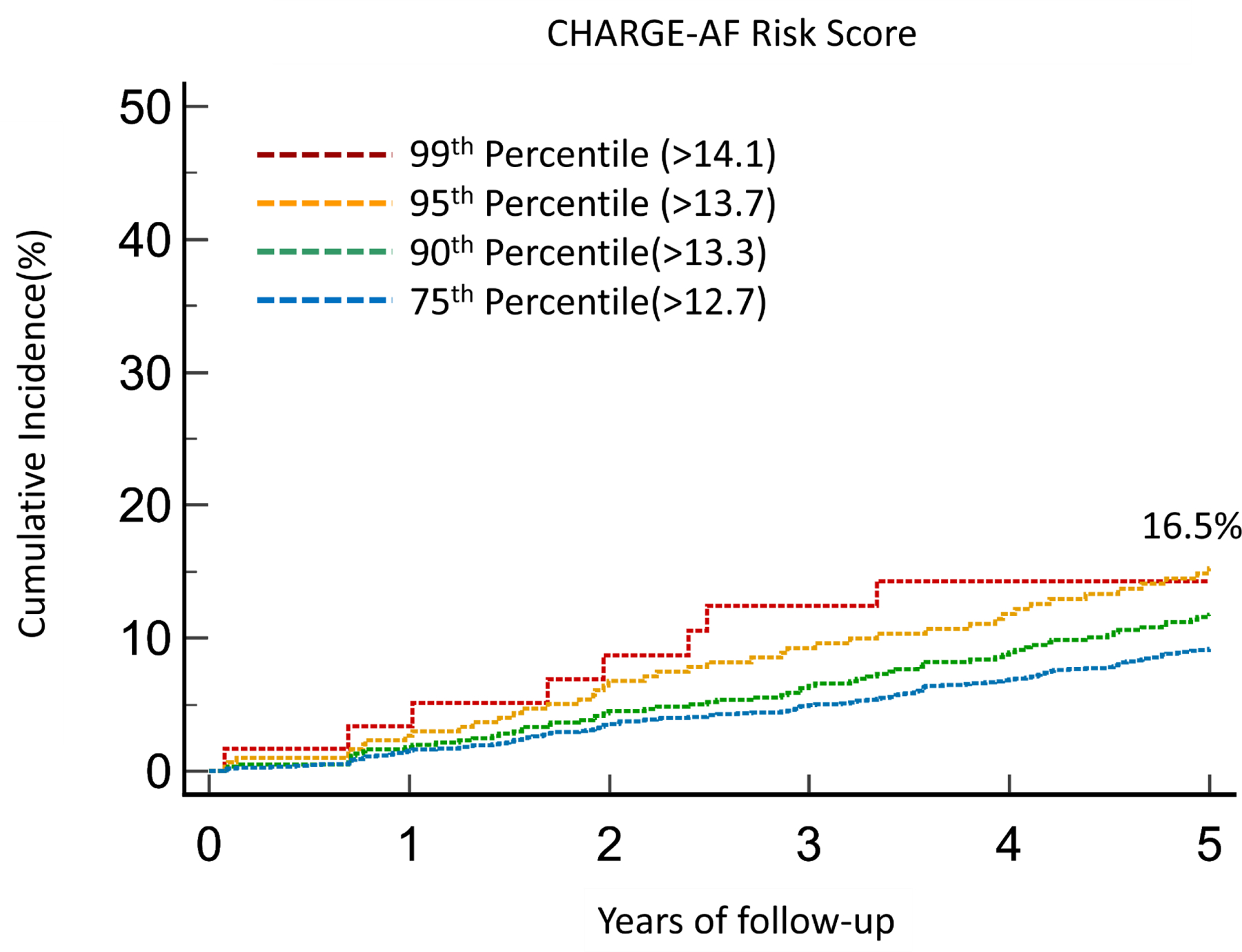
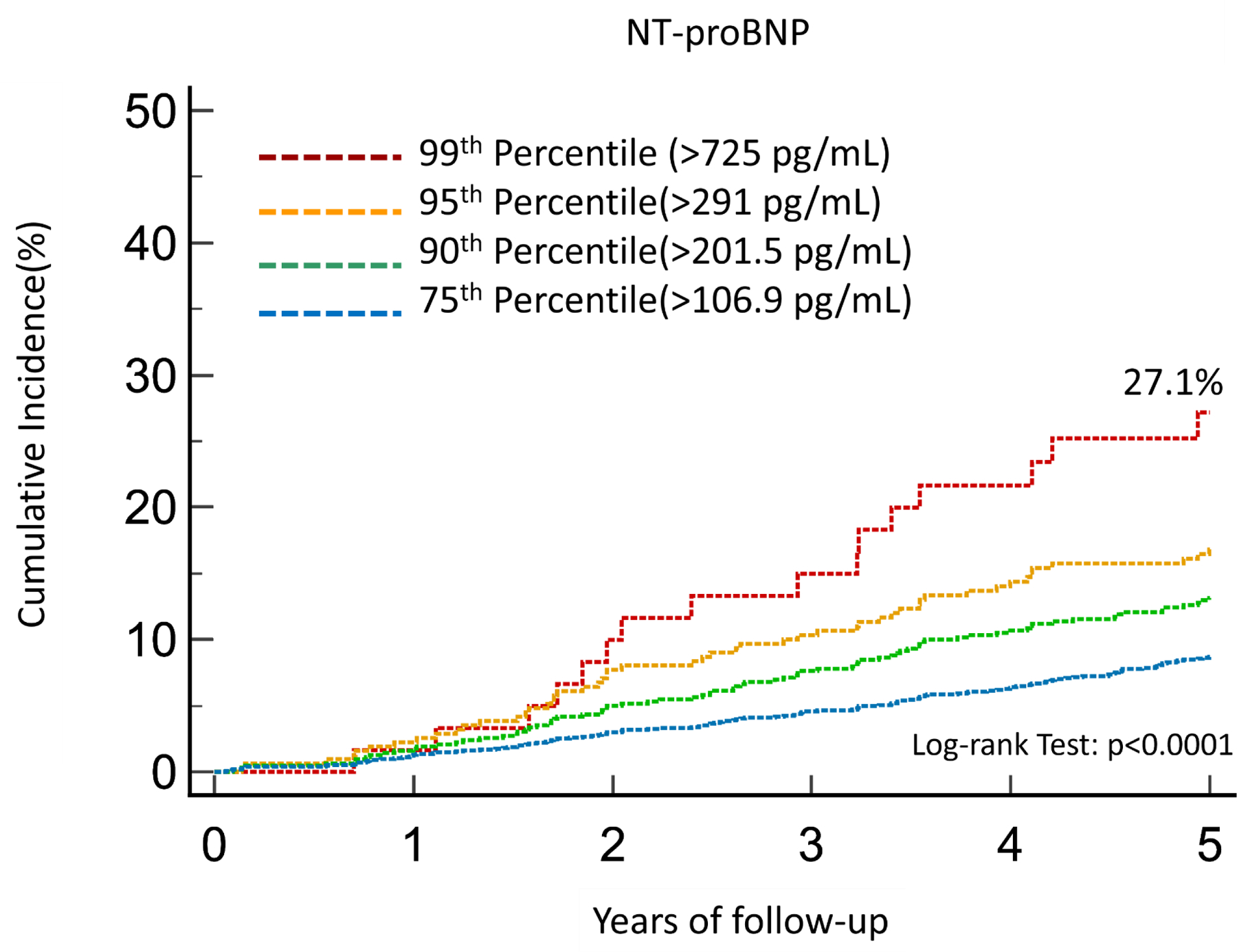
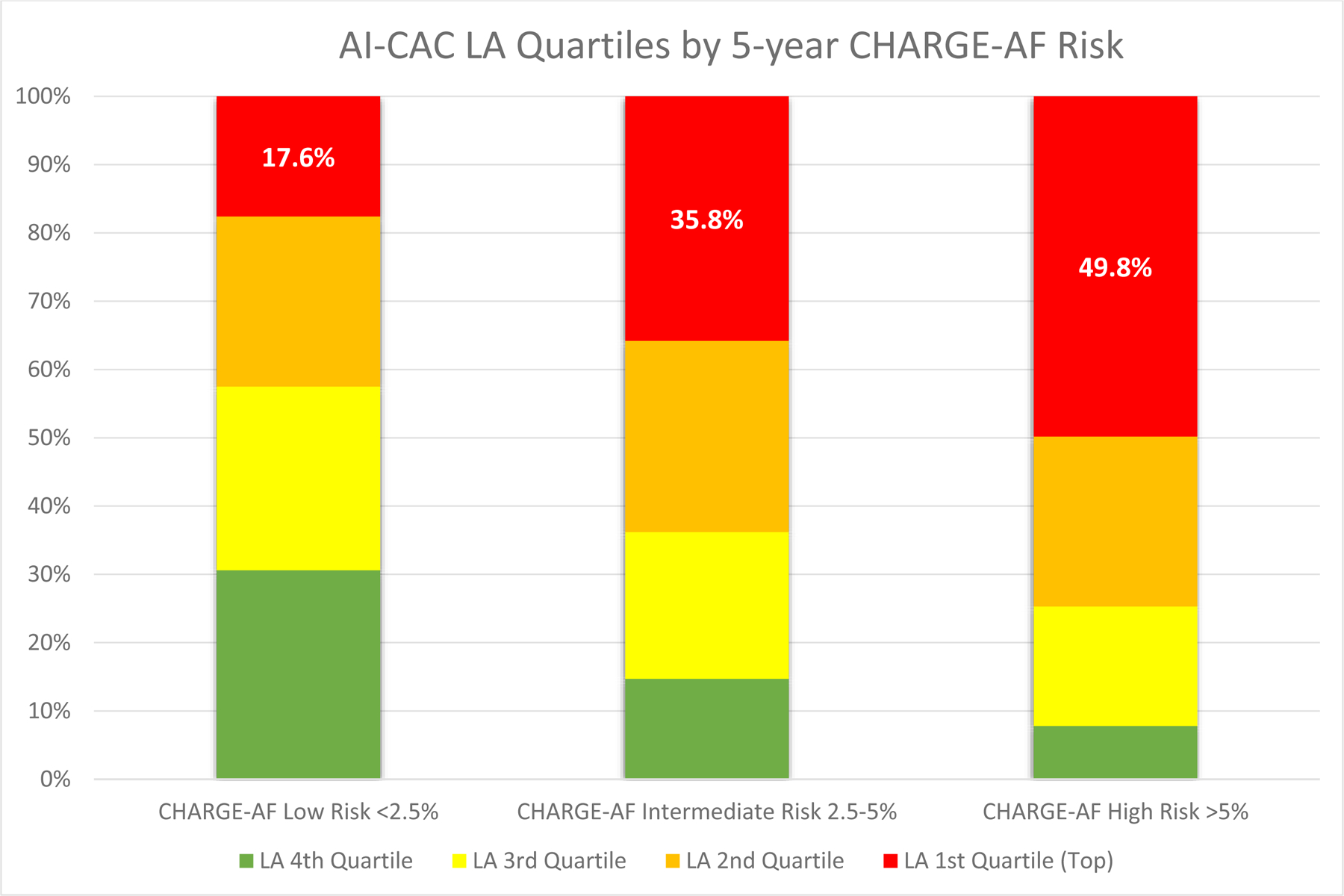
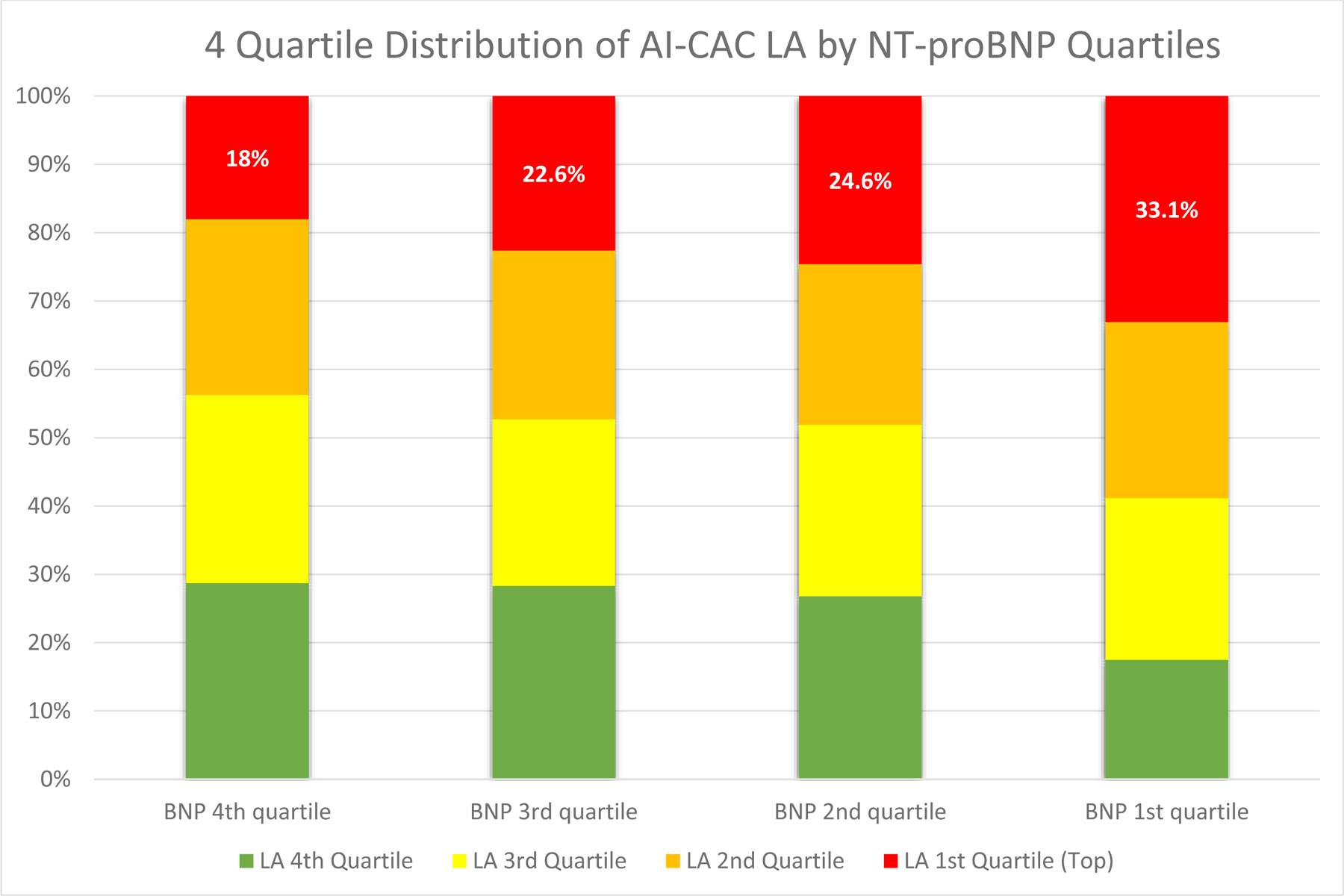
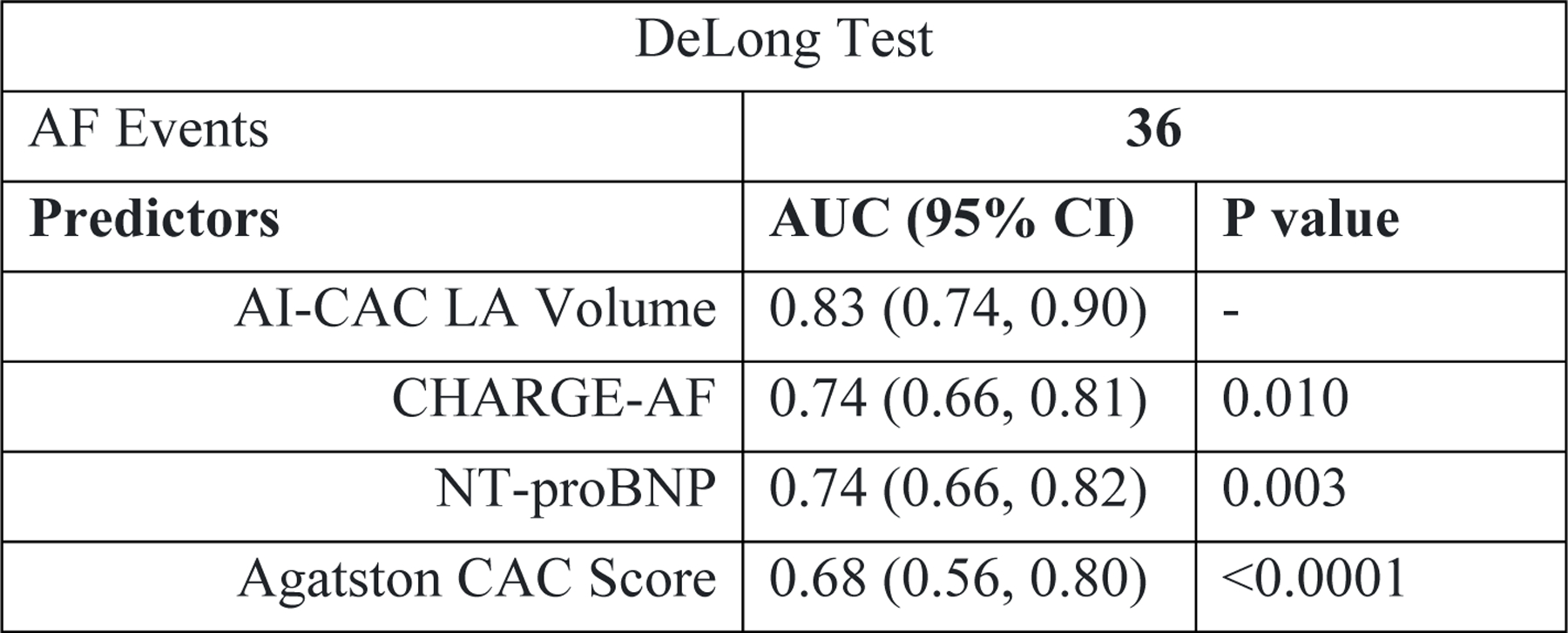
Results: At 1,2,3,4, and 5 years follow-up 36, 77, 123, 182, and 236 cases of AF were identified, respectively. The AUC for AI-CAC LA volume was significantly higher than CHARGE-AF for Years 1, 2, and 3 (0.83 vs. 0.74, 0.84 vs. 0.80, and 0.81 vs. 0.78, respectively, all p < 0.05), but similar for Years 4 and 5, and significantly higher than NT-proBNP at Years 1-5 (all p < 0.01), but not for combined CHARGE-AF and NT-proBNP at any year. AI-CAC LA significantly improved the continuous Net Reclassification Index for prediction of AF over years 1-5 when added to CHARGE-AF Risk Score (0.60, 0.28, 0.32, 0.19, 0.24), and NT-proBNP (0.68, 0.44, 0.42, 0.30, 0.37) (all p < 0.01).
Conclusion: AI-CAC LA volume enabled prediction of AF as early as one year and significantly improved on risk classification of CHARGE-AF Risk Score and NT-proBNP.
Keywords: Artificial intelligence; Atrial fibrillation; CHARGE-AF; Coronary artery calcium; Left atrial volume; NT-proBNP.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest Summary:
Several members of the writing group are inventors of the AI tool mentioned in this paper. Dr. Naghavi is the founder of HeartLung.AI. Dr. Reeves, Dr. Atlas, Dr. Yankelevitz, Dr, Wong, and Dr. Li are consultants for HeartLung.AI. Chenyu Zhang is a research contractor of HeartLung.AI. Kyle Atlas is a graduate research associate of HeartLung.AI. The remaining authors have nothing to disclose.
Figures
Update of
-
AI-enabled Left Atrial Volumetry in Cardiac CT Scans Improves CHARGE-AF and Outperforms NT-ProBNP for Prediction of Atrial Fibrillation in Asymptomatic Individuals: Multi-Ethnic Study of Atherosclerosis.medRxiv [Preprint]. 2024 Jan 24:2024.01.22.24301384. doi: 10.1101/2024.01.22.24301384. medRxiv. 2024. Update in: J Cardiovasc Comput Tomogr. 2024 Jul-Aug;18(4):383-391. doi: 10.1016/j.jcct.2024.04.005. PMID: 38343816 Free PMC article. Updated. Preprint.
Similar articles
-
AI-Enabled CT Cardiac Chamber Volumetry Predicts Atrial Fibrillation and Stroke Comparable to MRI.JACC Adv. 2024 Nov 15;3(11):101300. doi: 10.1016/j.jacadv.2024.101300. eCollection 2024 Nov. JACC Adv. 2024. PMID: 39741645 Free PMC article.
-
AI-enabled cardiac chambers volumetry in coronary artery calcium scans (AI-CACTM) predicts heart failure and outperforms NT-proBNP: The multi-ethnic study of Atherosclerosis.J Cardiovasc Comput Tomogr. 2024 Jul-Aug;18(4):392-400. doi: 10.1016/j.jcct.2024.04.006. Epub 2024 Apr 24. J Cardiovasc Comput Tomogr. 2024. PMID: 38664073 Free PMC article.
-
AI-enabled Left Atrial Volumetry in Cardiac CT Scans Improves CHARGE-AF and Outperforms NT-ProBNP for Prediction of Atrial Fibrillation in Asymptomatic Individuals: Multi-Ethnic Study of Atherosclerosis.medRxiv [Preprint]. 2024 Jan 24:2024.01.22.24301384. doi: 10.1101/2024.01.22.24301384. medRxiv. 2024. Update in: J Cardiovasc Comput Tomogr. 2024 Jul-Aug;18(4):383-391. doi: 10.1016/j.jcct.2024.04.005. PMID: 38343816 Free PMC article. Updated. Preprint.
-
The comparative and added prognostic value of biomarkers to the Revised Cardiac Risk Index for preoperative prediction of major adverse cardiac events and all-cause mortality in patients who undergo noncardiac surgery.Cochrane Database Syst Rev. 2021 Dec 21;12(12):CD013139. doi: 10.1002/14651858.CD013139.pub2. Cochrane Database Syst Rev. 2021. PMID: 34931303 Free PMC article.
-
The effectiveness and cost-effectiveness of computed tomography screening for coronary artery disease: systematic review.Health Technol Assess. 2006 Oct;10(39):iii-iv, ix-x, 1-41. doi: 10.3310/hta10390. Health Technol Assess. 2006. PMID: 17018228
Cited by
-
AI-enabled Cardiac Chambers Volumetry and Calcified Plaque Characterization in Coronary Artery Calcium (CAC) Scans (AI-CAC) Significantly Improves on Agatston CAC Score for Predicting All Cardiovascular Events: The Multi-Ethnic Study of Atherosclerosis.Res Sq [Preprint]. 2024 Jun 20:rs.3.rs-4433105. doi: 10.21203/rs.3.rs-4433105/v1. Res Sq. 2024. Update in: NPJ Digit Med. 2024 Nov 5;7(1):309. doi: 10.1038/s41746-024-01308-0. PMID: 38947043 Free PMC article. Updated. Preprint.
-
Baseline atrial volume indices and major adverse cardiac events following thoracic radiotherapy.Front Cardiovasc Med. 2025 Jun 3;12:1560922. doi: 10.3389/fcvm.2025.1560922. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40529555 Free PMC article.
-
AI-enabled opportunistic measurement of liver steatosis in coronary artery calcium scans predicts cardiovascular events and all-cause mortality: an AI-CVD study within the Multi-Ethnic Study of Atherosclerosis (MESA).BMJ Open Diabetes Res Care. 2025 Apr 12;13(2):e004760. doi: 10.1136/bmjdrc-2024-004760. BMJ Open Diabetes Res Care. 2025. PMID: 40221147 Free PMC article.
-
AI-Enabled CT Cardiac Chamber Volumetry Predicts Atrial Fibrillation and Stroke Comparable to MRI.JACC Adv. 2024 Nov 15;3(11):101300. doi: 10.1016/j.jacadv.2024.101300. eCollection 2024 Nov. JACC Adv. 2024. PMID: 39741645 Free PMC article.
-
AI-enabled cardiac chambers volumetry in coronary artery calcium scans (AI-CACTM) predicts heart failure and outperforms NT-proBNP: The multi-ethnic study of Atherosclerosis.J Cardiovasc Comput Tomogr. 2024 Jul-Aug;18(4):392-400. doi: 10.1016/j.jcct.2024.04.006. Epub 2024 Apr 24. J Cardiovasc Comput Tomogr. 2024. PMID: 38664073 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
- 75N92020D00002/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- 75N92020D00001/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- 75N92020D00005/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- 75N92020D00003/HL/NHLBI NIH HHS/United States
- R42 AR070713/AR/NIAMS NIH HHS/United States
- R01 HL146666/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- 75N92020D00004/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- 75N92020D00007/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- 75N92020D00006/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
