

Respiratory drive heterogeneity associated with systemic inflammation and vascular permeability in acute respiratory distress syndrome
- PMID: 38654391
- PMCID: PMC11036740
- DOI: 10.1186/s13054-024-04920-4
Respiratory drive heterogeneity associated with systemic inflammation and vascular permeability in acute respiratory distress syndrome
Abstract
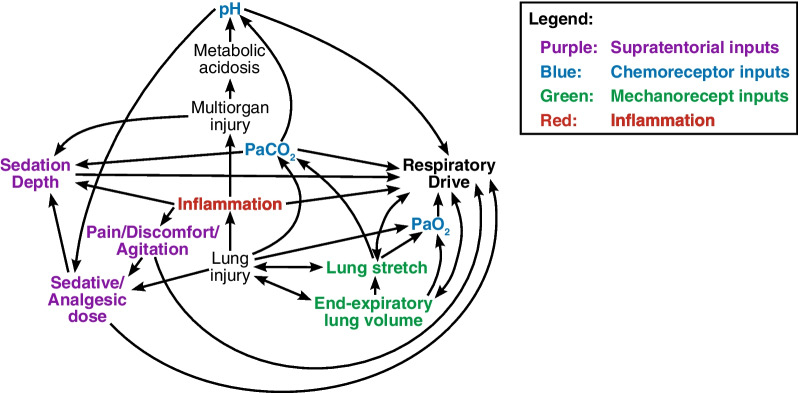
Background: In acute respiratory distress syndrome (ARDS), respiratory drive often differs among patients with similar clinical characteristics. Readily observable factors like acid-base state, oxygenation, mechanics, and sedation depth do not fully explain drive heterogeneity. This study evaluated the relationship of systemic inflammation and vascular permeability markers with respiratory drive and clinical outcomes in ARDS.
Methods: ARDS patients enrolled in the multicenter EPVent-2 trial with requisite data and plasma biomarkers were included. Neuromuscular blockade recipients were excluded. Respiratory drive was measured as PES0.1, the change in esophageal pressure during the first 0.1 s of inspiratory effort. Plasma angiopoietin-2, interleukin-6, and interleukin-8 were measured concomitantly, and 60-day clinical outcomes evaluated.
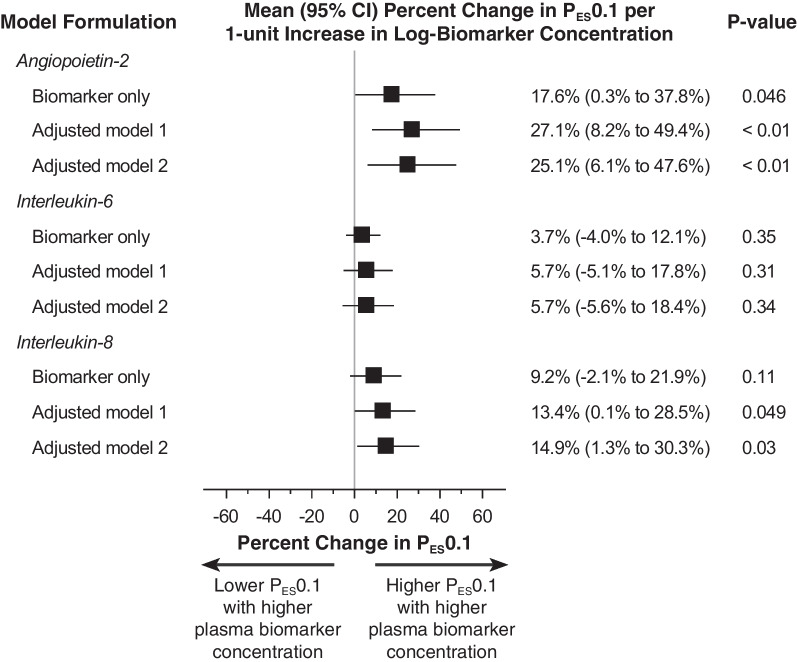
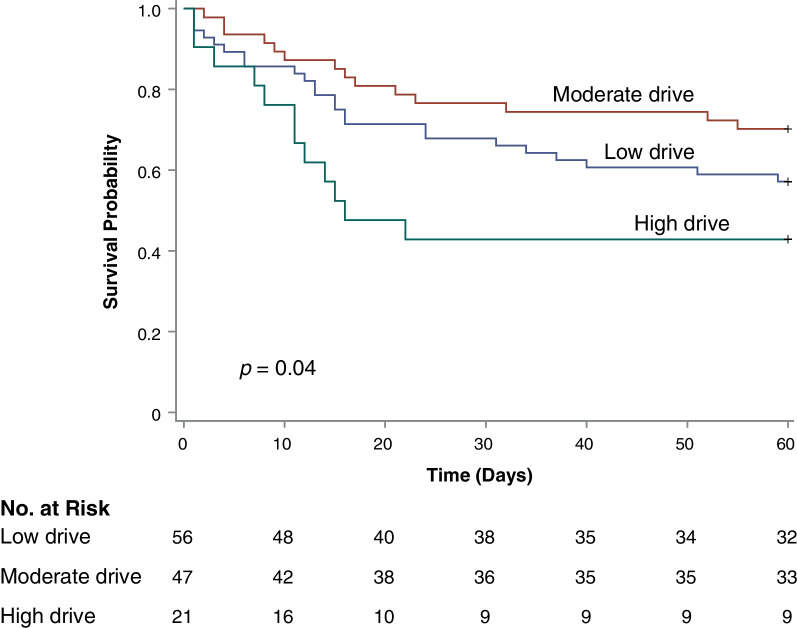
Results: 54.8% of 124 included patients had detectable respiratory drive (PES0.1 range of 0-5.1 cm H2O). Angiopoietin-2 and interleukin-8, but not interleukin-6, were associated with respiratory drive independently of acid-base, oxygenation, respiratory mechanics, and sedation depth. Sedation depth was not significantly associated with PES0.1 in an unadjusted model, or after adjusting for mechanics and chemoreceptor input. However, upon adding angiopoietin-2, interleukin-6, or interleukin-8 to models, lighter sedation was significantly associated with higher PES0.1. Risk of death was less with moderate drive (PES0.1 of 0.5-2.9 cm H2O) compared to either lower drive (hazard ratio 1.58, 95% CI 0.82-3.05) or higher drive (2.63, 95% CI 1.21-5.70) (p = 0.049).
Conclusions: Among patients with ARDS, systemic inflammatory and vascular permeability markers were independently associated with higher respiratory drive. The heterogeneous response of respiratory drive to varying sedation depth may be explained in part by differences in inflammation and vascular permeability.
Keywords: Acute respiratory distress syndrome; Hypnotics and sedatives; Mechanical ventilation; Respiratory mechanics; Work of breathing.
© 2024. The Author(s).
Conflict of interest statement
The authors declare they have no competing interests directly related to this study. Unrelated to this study, the authors provide the following disclosures. Dr. Baedorf-Kassis reports receiving honoraria and travel reimbursement from Hamilton Medical for presenting at continuing education workshops. Dr. Dzierba reports serving as a Council Member for the Society of Critical Care Medicine. Dr. Gong reports fees from Endpoint for serving on the scientific advisory panel, fees from Regeneron for serving on the data safety monitoring board of a clinical trial, and serves on the Executive Committee for the American Thoracic Society. Dr. Beitler reports prior consulting fees from Sedana Medical, Global Blood Therapeutics, Biomarck, and Arrowhead for work on advisory committees, and fees from Hamilton Medical for work as medical monitor of a clinical trial.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
