

The sequential antifracturative treatment: a meta-analysis of randomized clinical trials
- PMID: 38654732
- PMCID: PMC11036926
- DOI: 10.1177/1759720X241234584
The sequential antifracturative treatment: a meta-analysis of randomized clinical trials
Abstract
Background: Subjects with a fragility fracture have an increased risk of a new fracture and should receive effective strategies to prevent new events. The medium-term to long-term strategy should be scheduled by considering the mechanisms of action in therapy and the estimated fracture risk.
Objective: A systematic review was conducted to evaluate the sequential strategy in patients with or at risk of a fragility fracture in the context of the development of the Italian Guidelines.
Design: Systematic review and meta-analysis.
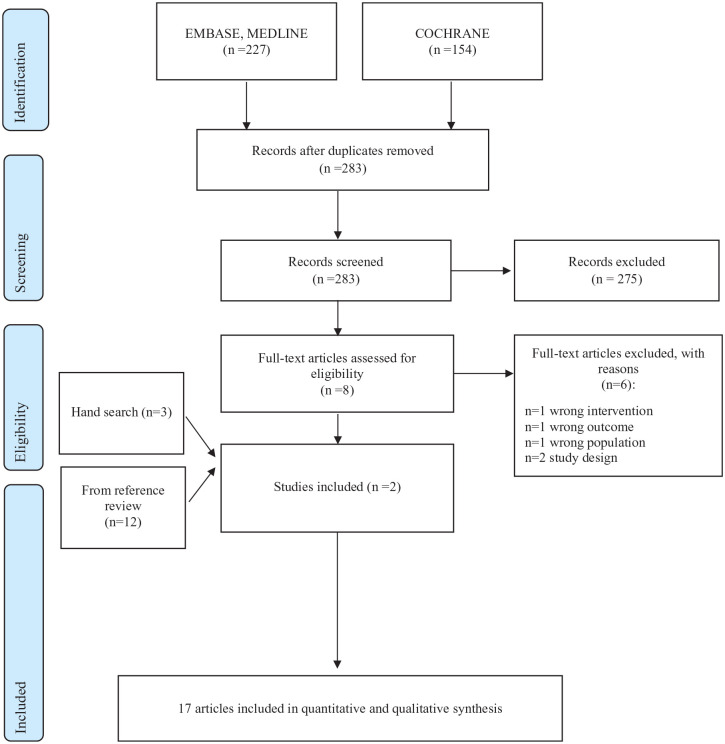
Data sources and methods: PubMed, Embase, and the Cochrane Library were investigated up to February 2021 to update the search of a recent systematic review. Randomized clinical trials (RCTs) that analyzed the sequential therapy of antiresorptive, anabolic treatment, or placebo in patients with or at risk of a fragility fracture were eligible. Three authors independently extracted data and appraised the risk of bias in the included studies. The quality of evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation methodology. Effect sizes were pooled in a meta-analysis using fixed-effects models. The primary outcome was the risk of refracture, while the secondary outcome was the bone mineral density (BMD) change.
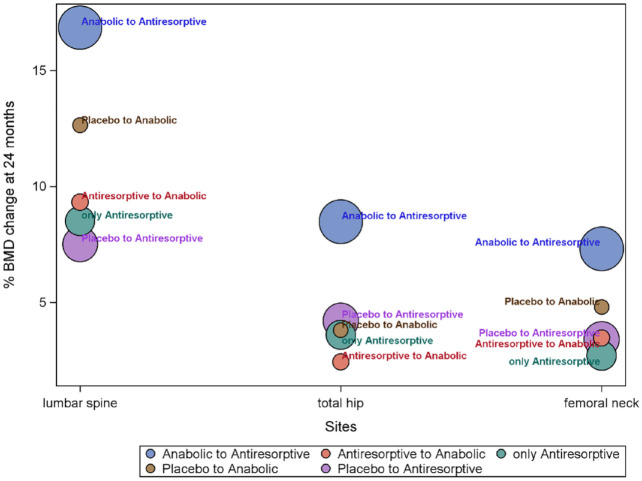
Results: In all, 17 RCTs, ranging from low to high quality, met our inclusion criteria. A significantly reduced risk of fracture was detected at (i) 12 or 24 months after the switch from romosozumab to denosumab versus placebo to denosumab; (ii) 30 months from teriparatide to bisphosphonates versus placebo to bisphosphonates; and (iii) 12 months from romosozumab to alendronate versus the only alendronate therapy (specifically for vertebral fractures). In general, at 2 years after the switch from anabolic to antiresorptive drugs, a weighted BMD was increased at the lumbar spine, total hip, and femoral neck site.
Conclusion: The Task Force formulated recommendations on sequential therapy, which is the first treatment with anabolic drugs or 'bone builders' in patients with very high or imminent risk of fracture.
Keywords: anabolic; antiresorptive; fragility fracture; sequential therapy; systematic review.
Plain language summary
A systematic review to evaluate the sequential therapy of antiresorptive (denosumab and bisphosphonate, such as alendronate, minodronate, risedronate, and etidronate), anabolic treatment (such as romosozumab, teriparatide), or placebo in patients with or at risk of a fragility fracture in the context of the development of the Italian Guidelines Subjects with previous fragility fractures should promptly receive effective strategies to prevent the risk of subsequent events. Indeed, patients with a fragility fracture have a doubled risk of a new fracture. For this reason, it is essential to provide adequate sequential therapy based on the mechanisms and the rapidity of action. A systematic review was performed to identify the sequential strategy in patients at high- or imminent-risk of (re)fracture and to support the Panel of the Italian Fragility Fracture Guideline in formulating recommendations. Our systematic review included seventeen studies mostly focused on women and enabled us to strongly recommend the anabolic drugs as first-line treatment. Specifically, for the sequential therapy from anabolic to antiresorptive treatment, there was a significant reduction in the risk of different types of fractures after the switch from romosozumab to denosumab versus placebo to denosumab. These findings were confirmed at 24 months after the switch. Considering the sequential treatment from antiresorptive to anabolic medications, there was a decreased risk of fracture 12 months after the switch from placebo to teriparatide versus bisphosphonate or antiresorptive to teriparatide. Moreover, a greater bone mineral density increase after the switch from anabolic to antiresorptive medications was shown in the lumbar spine, total hip, and femoral neck. The results of this systematic review and meta-analysis confirm that initial treatment with anabolic drugs produces substantial bone mineral density improvements, and the transition to antiresorptive drugs can preserve or even amplify the acquired benefit. These findings support the choice to treat very high-risk individuals with anabolic drugs first, followed by antiresorptive drugs.
© The Author(s), 2024.
Conflict of interest statement
GA declares personal fees from Theramex, Amgen, BMS, Lilly, Fresenius Kabi, and Galapagos. LC declares personal fees from UCB Pharma, Abiogen Pharma, Bruno Farmaceutici, Sandoz, and Metagenics. DG has received honoraria as a consultant for Eli-Lilly, Organon, and MSD Italia. SG has received honoraria as a consultant for UCB Pharma. SM has received honoraria as a consultant for UCB, Eli-Lilly, and Amgen. MLB has received (i) honoraria from Amgen, Bruno Farmaceutici, Calcilytix, Kyowa Kirin, UCB, (ii) grants and/or speaker: Abiogen, Alexion, Amgen, Bruno Farmaceutici, Echolight, Eli Lilly, Kyowa Kirin, SPA, Theramex, UCB Pharma, (iii) consultant: Alexion, Amolyt, Bruno Farmaceutici, Calcilytix, Kyowa Kirin, and UCB Pharma. GC received research support from the European Community (EC), the Italian Agency of Drug (AIFA), and the Italian Ministry for University and Research (MIUR). He took part in a variety of projects that were funded by pharmaceutical companies (i.e. Novartis, GSK, Roche, AMGEN, and BMS). He also received honoraria as a member of the Advisory Board from Roche. No other potential conflicts of interest relevant to this article were disclosed. MR declares personal fees from Amgen, ABBvie, BMS, Eli Lilly, Galapagos, Menarini, Novartis, Pfizer, Sandoz, Theramex, and UCB outside the submitted work. RM took part in a project funded by Abiogen Pharma. GI received honoraria as a speaker from Eli-Lilly, Menarini, and UCB Pharma. The other authors declare that they have no conflict of interest. All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author).
Figures
References
-
- Kanis JA, Johnell O, De Laet C, et al.. A meta-analysis of previous fracture and subsequent fracture risk. Bone 2004; 35: 375–382. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
