

Dual-energy X-ray absorptiometry derived knee shape may provide a useful imaging biomarker for predicting total knee replacement: Findings from a study of 37,843 people in UK Biobank
- PMID: 38655015
- PMCID: PMC11035060
- DOI: 10.1016/j.ocarto.2024.100468
Dual-energy X-ray absorptiometry derived knee shape may provide a useful imaging biomarker for predicting total knee replacement: Findings from a study of 37,843 people in UK Biobank
Abstract
Objective: We aimed to create an imaging biomarker for knee shape using knee dual-energy x-ray absorptiometry (DXA) scans and investigate its potential association with subsequent total knee replacement (TKR), independently of radiographic features of knee osteoarthritis and established risk factors.
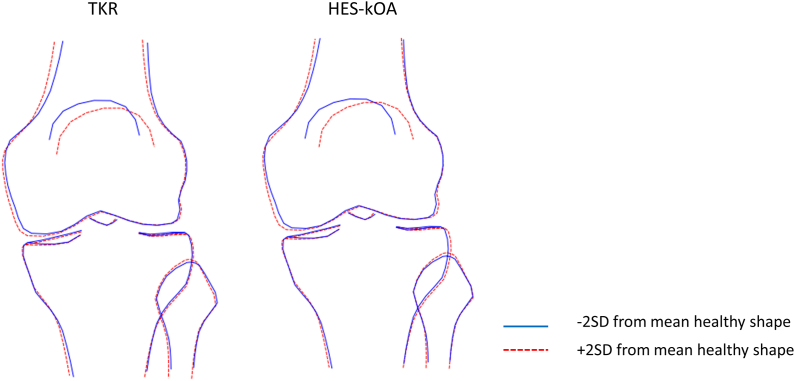
Methods: Using a 129-point statistical shape model, knee shape (expressed as a B-score) and minimum joint space width (mJSW) of the medial joint compartment (binarized as above or below the first quartile) were derived. Osteophytes were manually graded in a subset of images and an overall score was assigned. Cox proportional hazards models were used to examine the associations of B-score, mJSW and osteophyte score with TKR risk, adjusting for age, sex, height and weight.
Results: The analysis included 37,843 individuals (mean age 63.7 years). In adjusted models, B-score was associated with TKR: each unit increase in B-score, reflecting one standard deviation from the mean healthy shape, corresponded to a hazard ratio (HR) of 2.25 (2.08, 2.43), while a lower mJSW had a HR of 2.28 (1.88, 2.77). Among the 6719 images scored for osteophytes, mJSW was replaced by osteophyte score in the most strongly predictive model for TKR. In ROC analyses, a model combining B-score, osteophyte score, and demographics outperformed a model including demographics alone (AUC = 0.87 vs 0.73).
Conclusions: Using statistical shape modelling, we derived a DXA-based imaging biomarker for knee shape that was associated with kOA progression. When combined with osteophytes and demographic data, this biomarker may help identify individuals at high risk of TKR, facilitating targeted interventions.
Keywords: Knee shape; Osteoarthritis; Osteophytes; Statistical shape modelling.
© 2024 The Authors.
Conflict of interest statement
The other authors have declared no conflicts of interest. For the purpose of open access, the author has applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission. We confirm that there are no conflicts of interest associated with this manuscript, including any financial support or benefits from commercial sources.
Figures



References
-
- Hannan M.T., Felson D.T., Pincus T. Analysis of the discordance between radiographic changes and knee pain in osteoarthritis of the knee. J. Rheumatol. 2000;27(6):1513–1517. - PubMed
-
- Brouwer G.M., van Tol A.W., Bergink A.P., Belo J.N., Bernsen R.M., Reijman M., et al. Association between valgus and varus alignment and the development and progression of radiographic osteoarthritis of the knee. Arthritis Rheum. 2007;56(4):1204–1211. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
