

Mechanisms of Injury Leading to Concussions in Collegiate Soccer Players: A CARE Consortium Study
- PMID: 38656160
- PMCID: PMC11823273
- DOI: 10.1177/03635465241240789
Mechanisms of Injury Leading to Concussions in Collegiate Soccer Players: A CARE Consortium Study
Abstract
Background: Few previous studies have investigated how different injury mechanisms leading to sport-related concussion (SRC) in soccer may affect outcomes.
Purpose: To describe injury mechanisms and evaluate injury mechanisms as predictors of symptom severity, return to play (RTP) initiation, and unrestricted RTP (URTP) in a cohort of collegiate soccer players.
Study design: Cohort study; Level of evidence, 2.
Methods: The Concussion Assessment, Research and Education (CARE) Consortium database was used. The mechanism of injury was categorized into head-to-ball, head-to-head, head-to-body, and head-to-ground/equipment. Baseline/acute injury characteristics-including Sports Concussion Assessment Tool-3 total symptom severity (TSS), loss of consciousness (LOC), and altered mental status (AMS); descriptive data; and recovery (RTP and URTP)-were compared. Multivariable regression and Weibull models were used to assess the predictive value of the mechanism of injury on TSS and RTP/URTP, respectively.
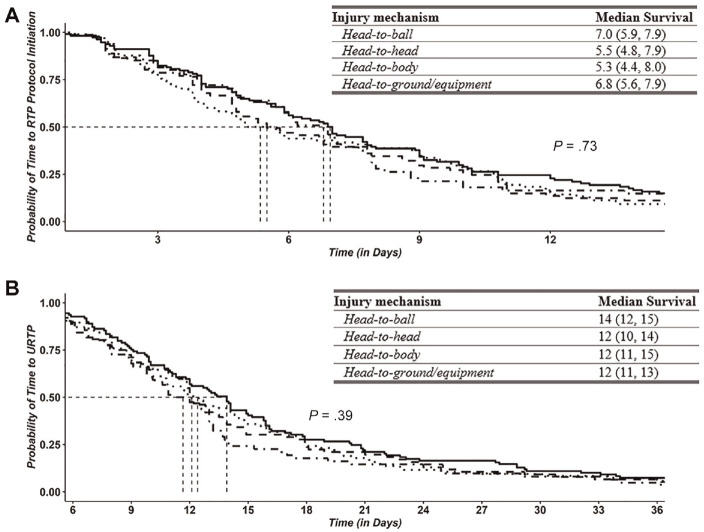
Results: Among 391 soccer SRCs, 32.7% were attributed to a head-to-ball mechanism, 27.9% to a head-to-body mechanism, 21.7% to a head-to-head mechanism, and 17.6% to a head-to-ground/equipment mechanism. Event type was significantly associated with injury mechanism [χ2(3) = 63; P < .001), such that more head-to-ball concussions occurred in practice sessions (n = 92 [51.1%] vs n = 36 [17.1%]) and more head-to-head (n = 65 [30.8%] vs n = 20 [11.1]) and head-to-body (n = 76 [36%] vs n = 33 [18.3%]) concussions occurred in competition. The primary position was significantly associated with injury mechanism [χ2(3) = 24; P < .004], with goalkeepers having no SRCs from the head-to-head mechanism (n = 0 [0%]) and forward players having the least head-to-body mechanism (n = 15 [19.2%]). LOC was also associated with injury mechanism (P = .034), with LOC being most prevalent in head-to-ground/equipment. Finally, AMS was most prevalent in head-to-ball (n = 54 [34.2%]) and head-to-body (n = 48 [30.4%]) mechanisms [χ2(3) = 9; P = .029]. In our multivariable models, the mechanism was not a predictor of TSS or RTP; however, it was associated with URTP (P = .044), with head-to-equipment/ground injuries resulting in the shortest mean number of days (14 ± 9.1 days) to URTP and the head-to-ball mechanism the longest (18.6 ± 21.6 days).
Conclusion: The mechanism of injury differed by event type and primary position, and LOC and AMS were different across mechanisms. Even though the mechanism of injury was not a significant predictor of acute symptom burden or time until RTP initiation, those with head-to-equipment/ground injuries spent the shortest time until URTP, and those with head-to-ball injuries had the longest time until URTP.
Keywords: outcome; return to play; soccer; sport-related concussion.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: This project was supported, in part, by the Grand Alliance Sport-Related Concussion Assessment, Research, and Education (CARE) Consortium, funded, in part by the National Collegiate Athletic Association (NCAA) and the DoD. The U.S. Army Medical Research Acquisition Activity is the awarding and administering acquisition office. This work was supported by the Office of the Assistant Secretary of Defense for Health Affairs through the Psychological Health and Traumatic Brain Injury Program under award No. W81XWH-14-2-0151. A.J.B. has been part of projects that have received funding from the DoD, the National Operating Committee on Standards from Athletic Equipment, the National Athletic Trainer's Association (NATA) Research and Education Foundation, and the NCAA. P.F.P. is an employee of the DoD and has previously received other DoD-related grants. T.W.M. has received research support from the NCAA, the US DoD, and the National Institutes of Health (NIH). He also reports textbook royalties from American Psychiatric Press Publishing Inc and serves on the Concussion Committee Scientific Advisory Board for the Australian Football League. M.A.M. has received research funding from the NIH, the Centers for Disease Control and Prevention (CDC), the DoD, the NCAA, the National Football League (NFL), and Abbott Laboratories. S.P.B. has received research funding from the NIH, the CDC, the DoD-USA Medical Research Acquisition Activity, the NCAA, the NATA Research and Education Foundation, the NFL/Under Armour/GE, Simbex, and ElmindA. He has consulted for US Soccer, US Cycling, the University of Calgary SHRed Concussions external advisory board, and medicolegal litigation. S.L.Z. is a member of the NFL Head, Neck, and Spine Committee. D.P.T. serves as a scientific advisor for HitIQ. He previously consulted for REACT Neuro Inc. He has a consulting practice in forensic neuropsychology, including expert testimony, involving individuals who have sustained mild traumatic brain injury (including former athletes). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures

References
-
- Blyth RJ, Alcock M, Tumilty DS. Why are female soccer players experiencing a concussion more often than their male counterparts? A scoping review. Phys Ther Sport. 2021;52:54-68. - PubMed
-
- Broglio SP, McCrea M, McAllister T, et al.. A national study on the effects of concussion in collegiate athletes and US military service academy members: The NCAA-DoD Concussion Assessment, Research and Education (CARE) consortium structure and methods. Sports Med Auckl NZ. 2017;47(7):1437-1451. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
