

A case of enormous retroperitoneal liposarcoma with prolapse from the left inguinal canal following hernia repair
- PMID: 38656390
- PMCID: PMC11043317
- DOI: 10.1186/s40792-024-01891-0
A case of enormous retroperitoneal liposarcoma with prolapse from the left inguinal canal following hernia repair
Abstract
Background: Liposarcomas represent ~9.8-16% of soft tissue sarcomas, with the extremities and retroperitoneum being the primary sites of occurrence. While liposarcoma in the inguinal region is uncommon, few reported cases originate from the retroperitoneum and protrude into the scrotum through the inguinal canal. Here, we present a case of a retroperitoneal liposarcoma with prolapse from the left inguinal canal into the scrotum following hernia repair with a mesh plug.
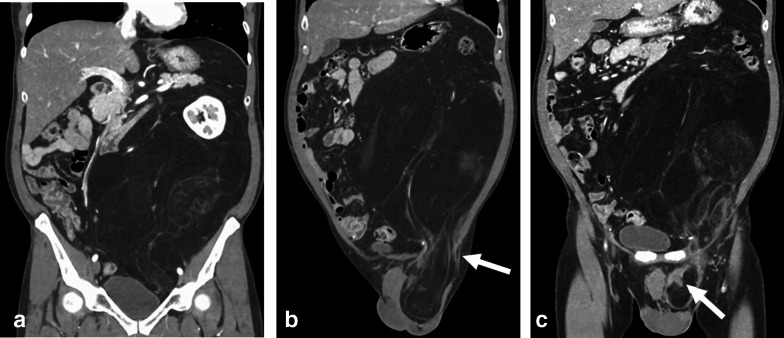
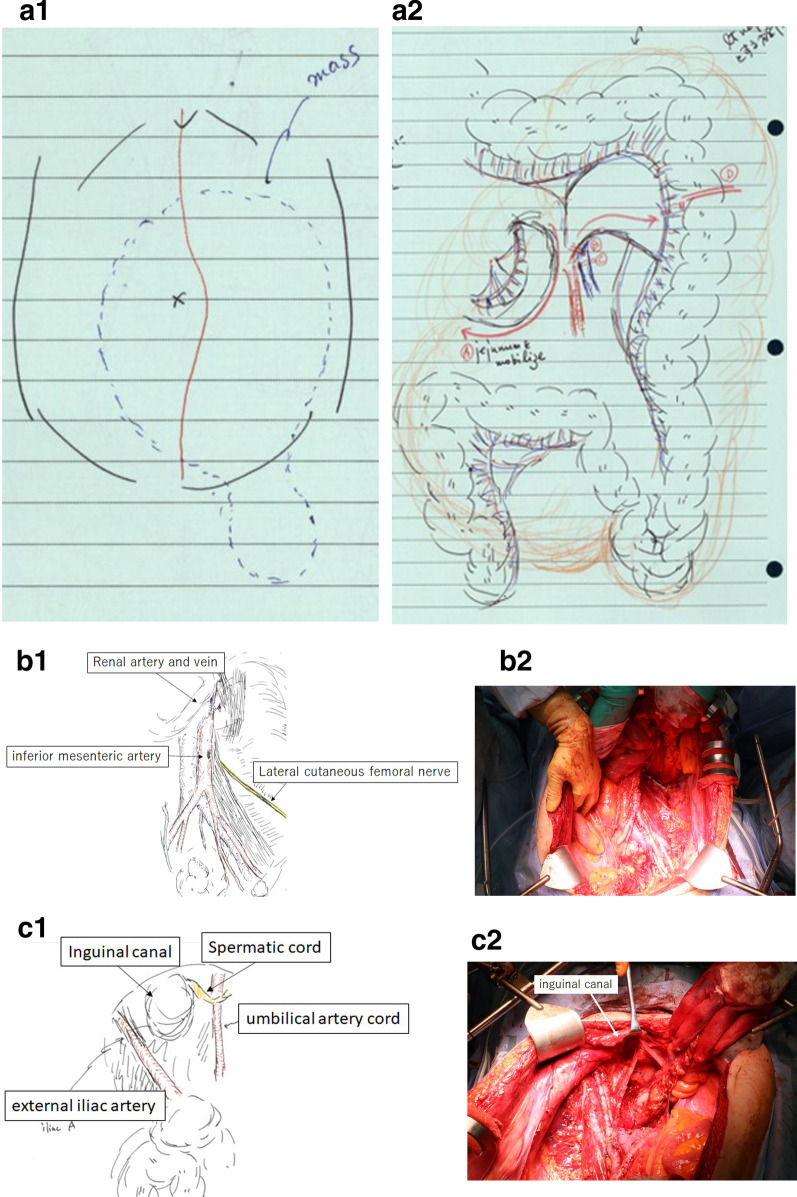
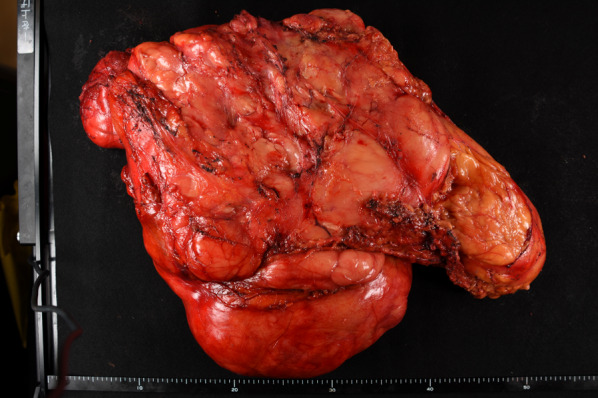
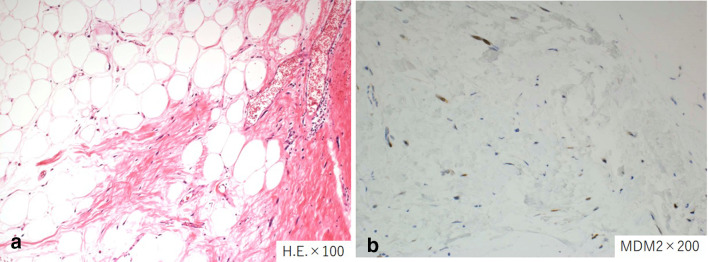
Case presentation: A 55-year-old male patient underwent a CT scan for a suspected recurrent inguinal hernia, which revealed a sizeable adipose-dense tumor by the left kidney extruded through the left inguinal canal surrounding the scrotum. The patient had undergone mesh plug repair for a left inguinal hernia at another hospital one year ago and noticed ipsilateral inguinal swelling after the hernia repair. The patient was referred to our hospital. The tumor resection was completed with combined resection of potentially involved organs: left side colon, left kidney, and left adrenal gland. Also, complete excision of the tumor was accomplished through surgical resection of the posterior wall of the inguinal canal, the mesh plug, and the tumor extending into the scrotum. Given the nearly complete absence of the inguinal canal's posterior wall and the anterior wall's torn state, sutures were employed to close the external obturator tenosynovitis. Additionally, the inguinal ligament was closed using a tension-free incision technique. Only a mesh was subsequently placed. The resected tumor measured 47 × 30 × 15 cm and 7.5 kg in weight. After surgical resection, a retroperitoneal liposarcoma diagnosis was established. After 2 years and 6 months following the surgical resection, no recurrence has been observed for either liposarcoma or inguinal hernia.
Conclusion: The previous inguinal hernia in this case must be a prolapse of retroperitoneal liposarcoma. Thus, it is recommended to conduct a preoperative examination, which should include a CT scan, since the presence of a fatty mass within the hernia may indicate the presence of a retroperitoneal liposarcoma. Even if a preoperative diagnosis cannot be made, a long-term prognosis can be expected if the retroperitoneal liposarcoma can be completely resected at reoperation.
Keywords: Inguinal hernia; Retroperitoneal; Sarcoma.
© 2024. The Author(s).
Conflict of interest statement
Not applicable.
Figures
Similar articles
-
Usefulness of laparoscopy in the management of incidentally discovered retroperitoneal liposarcoma mimicking inguinal hernia: A case report and literature review.Int J Surg Case Rep. 2020;72:79-84. doi: 10.1016/j.ijscr.2020.05.064. Epub 2020 Jun 3. Int J Surg Case Rep. 2020. PMID: 32516702 Free PMC article.
-
Pseudo-beer belly disguised and presenting as inguinal hernia swelling: a case of massive retroperitoneal liposarcoma.Front Med (Lausanne). 2025 May 2;12:1499764. doi: 10.3389/fmed.2025.1499764. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40385582 Free PMC article.
-
A case of retroperitoneal liposarcoma extending through the inguinal canal to the thigh and lesser trochanter.IJU Case Rep. 2023 Jun 16;6(4):257-261. doi: 10.1002/iju5.12600. eCollection 2023 Jul. IJU Case Rep. 2023. PMID: 37405036 Free PMC article.
-
Retroperitoneal Liposarcoma: A Concern in Inguinal Hernia Repair.JSLS. 2019 Jan-Mar;23(1):e2018.00064. doi: 10.4293/JSLS.2018.00064. JSLS. 2019. PMID: 30700965 Free PMC article.
-
Spermatic cord liposarcomas incidentally found during hernia surgery: is histology of any lipoma mandatory? A review of the literature.Acta Chir Belg. 2020 Apr;120(2):79-84. doi: 10.1080/00015458.2019.1689645. Epub 2019 Nov 12. Acta Chir Belg. 2020. PMID: 31690184 Review.
References
-
- Noguchi H, Naomoto Y, Haisa M, Yamatsuji T, Shigemitsu K, Uetsuka H, et al. Retroperitoneal liposarcoma presenting a indirect inguinal hernia. Acta Med Okayama. 2001;55(1):51–54. - PubMed
LinkOut - more resources
Full Text Sources
