

ESR Essentials: screening for breast cancer - general recommendations by EUSOBI
- PMID: 38656711
- PMCID: PMC11399176
- DOI: 10.1007/s00330-024-10740-5
ESR Essentials: screening for breast cancer - general recommendations by EUSOBI
Abstract
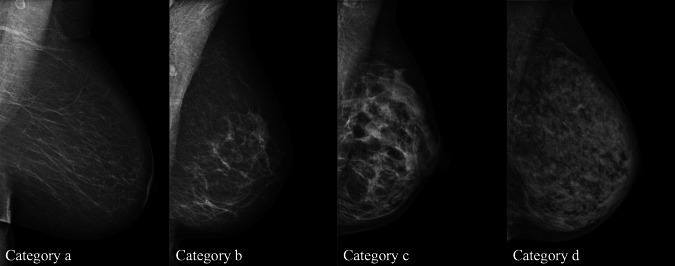
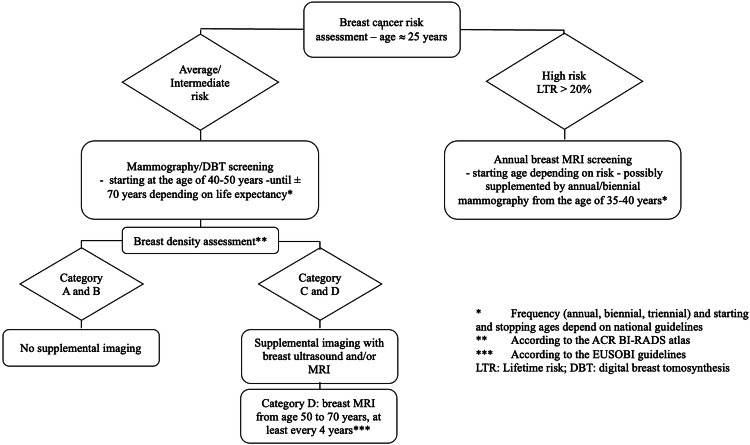
Breast cancer is the most frequently diagnosed cancer in women accounting for about 30% of all new cancer cases and the incidence is constantly increasing. Implementation of mammographic screening has contributed to a reduction in breast cancer mortality of at least 20% over the last 30 years. Screening programs usually include all women irrespective of their risk of developing breast cancer and with age being the only determining factor. This approach has some recognized limitations, including underdiagnosis, false positive cases, and overdiagnosis. Indeed, breast cancer remains a major cause of cancer-related deaths in women undergoing cancer screening. Supplemental imaging modalities, including digital breast tomosynthesis, ultrasound, breast MRI, and, more recently, contrast-enhanced mammography, are available and have already shown potential to further increase the diagnostic performances. Use of breast MRI is recommended in high-risk women and women with extremely dense breasts. Artificial intelligence has also shown promising results to support risk categorization and interval cancer reduction. The implementation of a risk-stratified approach instead of a "one-size-fits-all" approach may help to improve the benefit-to-harm ratio as well as the cost-effectiveness of breast cancer screening. KEY POINTS: Regular mammography should still be considered the mainstay of the breast cancer screening. High-risk women and women with extremely dense breast tissue should use MRI for supplemental screening or US if MRI is not available. Women need to participate actively in the decision to undergo personalized screening. KEY RECOMMENDATIONS: Mammography is an effective imaging tool to diagnose breast cancer in an early stage and to reduce breast cancer mortality (evidence level I). Until more evidence is available to move to a personalized approach, regular mammography should be considered the mainstay of the breast cancer screening. High-risk women should start screening earlier; first with yearly breast MRI which can be supplemented by yearly or biennial mammography starting at 35-40 years old (evidence level I). Breast MRI screening should be also offered to women with extremely dense breasts (evidence level I). If MRI is not available, ultrasound can be performed as an alternative, although the added value of supplemental ultrasound regarding cancer detection remains limited. Individual screening recommendations should be made through a shared decision-making process between women and physicians.
Keywords: Breast neoplasms; Early detection of cancer; Magnetic resonance imaging; Mammography; Ultrasonography (mammary).
© 2024. The Author(s).
Conflict of interest statement
P.C. is a member of the Scientific Editorial Board for
Figures
References
-
- IARC Cancer Today. International Agency for Research on Cancer Centers for disease Control and prevention Accessed September 7, 2023
-
- McCormack VA, dos Santos Silva I (2006) Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidemiol Biomarkers Prev 15:1159–1169 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
