

The Costs of Anonymization: Case Study Using Clinical Data
- PMID: 38657232
- PMCID: PMC11079766
- DOI: 10.2196/49445
The Costs of Anonymization: Case Study Using Clinical Data
Abstract
Background: Sharing data from clinical studies can accelerate scientific progress, improve transparency, and increase the potential for innovation and collaboration. However, privacy concerns remain a barrier to data sharing. Certain concerns, such as reidentification risk, can be addressed through the application of anonymization algorithms, whereby data are altered so that it is no longer reasonably related to a person. Yet, such alterations have the potential to influence the data set's statistical properties, such that the privacy-utility trade-off must be considered. This has been studied in theory, but evidence based on real-world individual-level clinical data is rare, and anonymization has not broadly been adopted in clinical practice.
Objective: The goal of this study is to contribute to a better understanding of anonymization in the real world by comprehensively evaluating the privacy-utility trade-off of differently anonymized data using data and scientific results from the German Chronic Kidney Disease (GCKD) study.
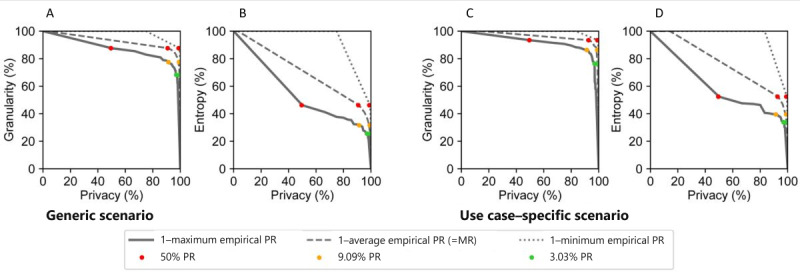
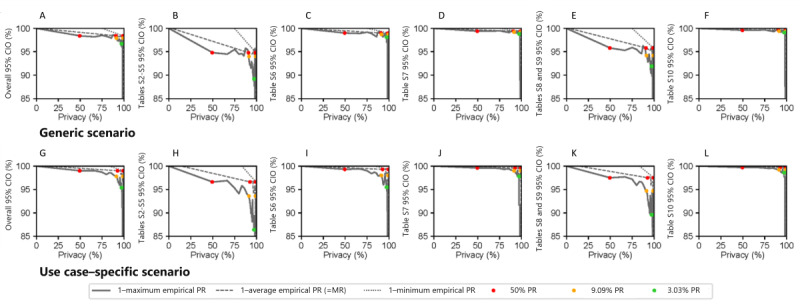
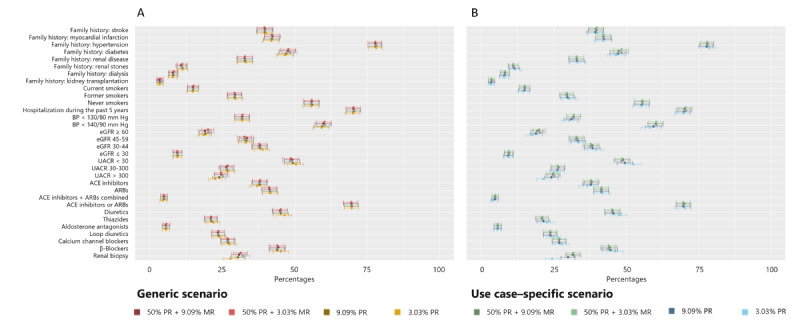
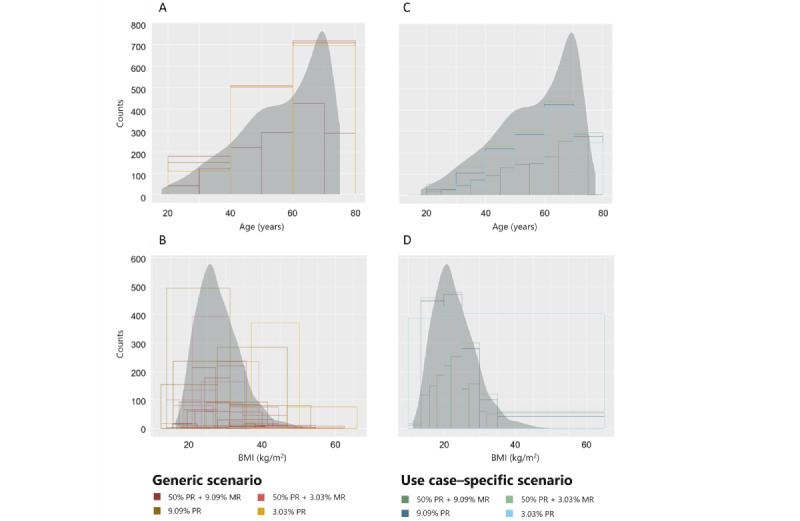
Methods: The GCKD data set extracted for this study consists of 5217 records and 70 variables. A 2-step procedure was followed to determine which variables constituted reidentification risks. To capture a large portion of the risk-utility space, we decided on risk thresholds ranging from 0.02 to 1. The data were then transformed via generalization and suppression, and the anonymization process was varied using a generic and a use case-specific configuration. To assess the utility of the anonymized GCKD data, general-purpose metrics (ie, data granularity and entropy), as well as use case-specific metrics (ie, reproducibility), were applied. Reproducibility was assessed by measuring the overlap of the 95% CI lengths between anonymized and original results.
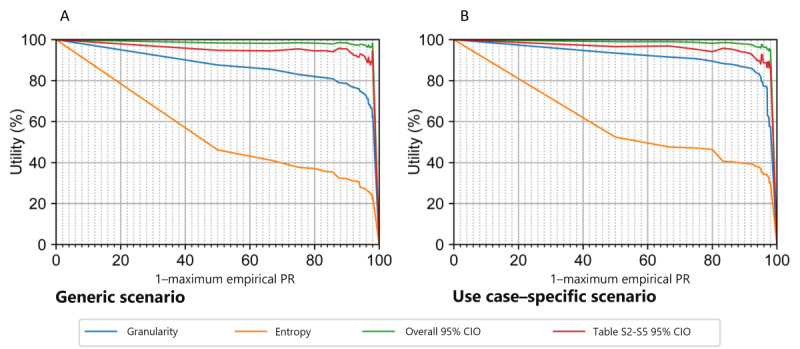
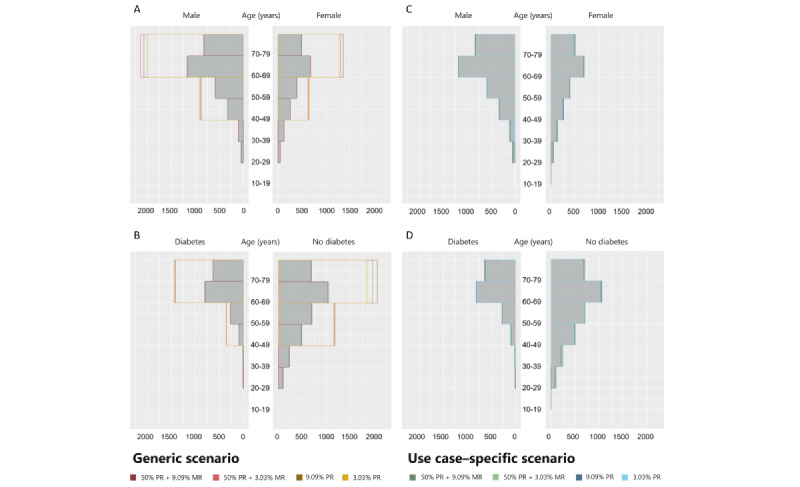
Results: Reproducibility measured by 95% CI overlap was higher than utility obtained from general-purpose metrics. For example, granularity varied between 68.2% and 87.6%, and entropy varied between 25.5% and 46.2%, whereas the average 95% CI overlap was above 90% for all risk thresholds applied. A nonoverlapping 95% CI was detected in 6 estimates across all analyses, but the overwhelming majority of estimates exhibited an overlap over 50%. The use case-specific configuration outperformed the generic one in terms of actual utility (ie, reproducibility) at the same level of privacy.
Conclusions: Our results illustrate the challenges that anonymization faces when aiming to support multiple likely and possibly competing uses, while use case-specific anonymization can provide greater utility. This aspect should be taken into account when evaluating the associated costs of anonymized data and attempting to maintain sufficiently high levels of privacy for anonymized data.
Trial registration: German Clinical Trials Register DRKS00003971; https://drks.de/search/en/trial/DRKS00003971.
International registered report identifier (irrid): RR2-10.1093/ndt/gfr456.
Keywords: anonymization; anonymized; confidentiality; data science; data sharing; deidentification; identification; medical informatics; privacy; privacy-enhancing technologies; privacy-utility trade-off; security.
©Lisa Pilgram, Thierry Meurers, Bradley Malin, Elke Schaeffner, Kai-Uwe Eckardt, Fabian Prasser, GCKD Investigators. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 24.04.2024.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Mansmann U, Locher C, Prasser F, Weissgerber T, Sax U, Posch M, Decullier E, Cristea IA, Debray TPA, Held L, Moher D, Ioannidis JPA, Ross JS, Ohmann C, Naudet F. Implementing clinical trial data sharing requires training a new generation of biomedical researchers. Nat Med. 2023;29(2):298–301. doi: 10.1038/s41591-022-02080-y. https://hal.science/hal-04010046 10.1038/s41591-022-02080-y - DOI - PubMed
-
- Egilman AC, Kapczynski A, McCarthy ME, Luxkaranayagam AT, Morten CJ, Herder M, Wallach JD, Ross JS. Transparency of regulatory data across the European Medicines Agency, Health Canada, and US Food and Drug Administration. J Law Med Ethics. 2021;49(3):456–485. doi: 10.1017/jme.2021.67.S107311052100067X - DOI - PubMed
-
- Naudet F, Siebert M, Pellen C, Gaba J, Axfors C, Cristea I, Danchev V, Mansmann U, Ohmann C, Wallach JD, Moher D, Ioannidis JPA. Medical journal requirements for clinical trial data sharing: ripe for improvement. PLoS Med. 2021;18(10):e1003844. doi: 10.1371/journal.pmed.1003844. https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1... PMEDICINE-D-20-02944 - DOI - PMC - PubMed
-
- Wilkinson MD, Dumontier M, Aalbersberg IJJ, Appleton G, Axton M, Baak A, Blomberg N, Boiten J, da Silva Santos LB, Bourne PE, Bouwman J, Brookes AJ, Clark T, Crosas M, Dillo I, Dumon O, Edmunds S, Evelo CT, Finkers R, Gonzalez-Beltran A, Gray AJG, Groth P, Goble C, Grethe JS, Heringa J, 't Hoen PAC, Hooft R, Kuhn T, Kok R, Kok J, Lusher SJ, Martone ME, Mons A, Packer AL, Persson B, Rocca-Serra P, Roos M, van Schaik R, Sansone S, Schultes E, Sengstag T, Slater T, Strawn G, Swertz MA, Thompson M, van der Lei J, van Mulligen E, Velterop J, Waagmeester A, Wittenburg P, Wolstencroft K, Zhao J, Mons B. The FAIR guiding principles for scientific data management and stewardship. Sci Data. 2016;3:160018. doi: 10.1038/sdata.2016.18. doi: 10.1038/sdata.2016.18.sdata201618 - DOI - PMC - PubMed
-
- EU General Data Protection Regulation (GDPR): Regulation (EU) 2016/679, Article 5(1)(c) Dsgvo-Portal. 2016. [2023-04-22]. https://www.dsgvo-portal.de/gdpr_article_5.php .
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
