

Immune mechanisms in the pathophysiology of hypertension
- PMID: 38658669
- PMCID: PMC12060254
- DOI: 10.1038/s41581-024-00838-w
Immune mechanisms in the pathophysiology of hypertension
Abstract
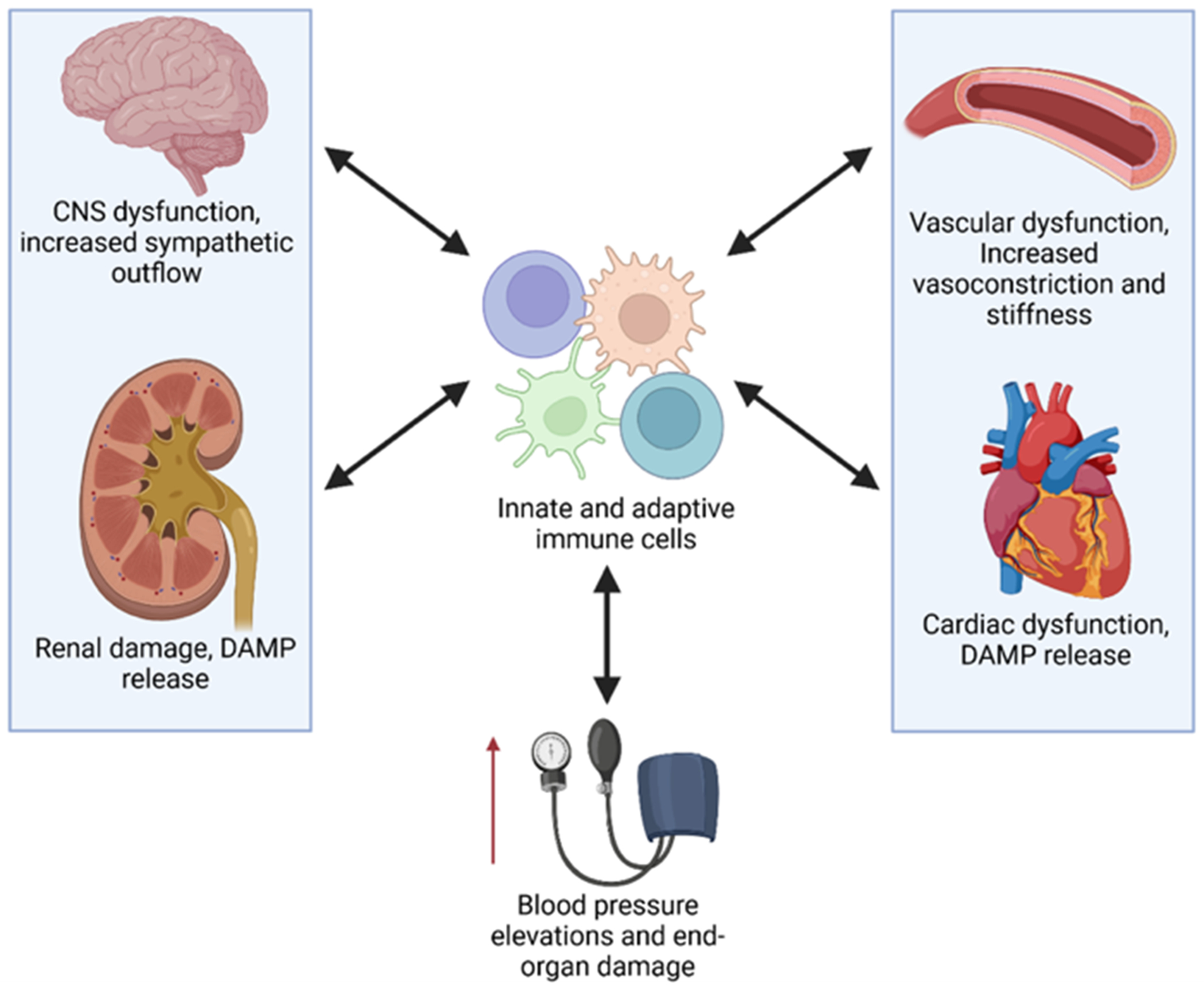
Hypertension is a leading risk factor for morbidity and mortality worldwide. Despite current anti-hypertensive therapies, most individuals with hypertension fail to achieve adequate blood pressure control. Moreover, even with adequate control, a residual risk of cardiovascular events and associated organ damage remains. These findings suggest that current treatment modalities are not addressing a key element of the underlying pathology. Emerging evidence implicates immune cells as key mediators in the development and progression of hypertension. In this Review, we discuss our current understanding of the diverse roles of innate and adaptive immune cells in hypertension, highlighting key findings from human and rodent studies. We explore mechanisms by which these immune cells promote hypertensive pathophysiology, shedding light on their multifaceted involvement. In addition, we highlight advances in our understanding of autoimmunity, HIV and immune checkpoints that provide valuable insight into mechanisms of chronic and dysregulated inflammation in hypertension.
© 2024. Springer Nature Limited.
Conflict of interest statement
Competing Interests
None
Figures


Similar articles
-
Recent Advances in Immunity and Hypertension.Am J Hypertens. 2017 Jul 1;30(7):643-652. doi: 10.1093/ajh/hpx011. Am J Hypertens. 2017. PMID: 28200062 Review.
-
The immunological basis of hypertension.Am J Hypertens. 2014 Nov;27(11):1327-37. doi: 10.1093/ajh/hpu142. Epub 2014 Aug 23. Am J Hypertens. 2014. PMID: 25150828 Free PMC article. Review.
-
Are the innate and adaptive immune systems setting hypertension on fire?Pharmacol Res. 2017 Mar;117:377-393. doi: 10.1016/j.phrs.2017.01.010. Epub 2017 Jan 16. Pharmacol Res. 2017. PMID: 28093357 Review.
-
Innate Immune Cells and Hypertension: Neutrophils and Neutrophil Extracellular Traps (NETs).Compr Physiol. 2021 Feb 12;11(1):1575-1589. doi: 10.1002/cphy.c200020. Compr Physiol. 2021. PMID: 33577121 Free PMC article. Review.
-
Hypertension: Do Inflammation and Immunity Hold the Key to Solving this Epidemic?Circ Res. 2021 Apr 2;128(7):908-933. doi: 10.1161/CIRCRESAHA.121.318052. Epub 2021 Apr 1. Circ Res. 2021. PMID: 33793336 Free PMC article. Review.
Cited by
-
A Multi-marker model based on serum IL-10 predicts response to conversion immunochemotherapy in gastric cancer patients: a retrospective cohort study.BMC Gastroenterol. 2025 Aug 27;25(1):621. doi: 10.1186/s12876-025-04136-y. BMC Gastroenterol. 2025. PMID: 40866830 Free PMC article.
-
Immunotherapy for hypertensive end-organ damage: a new therapeutic strategy.Essays Biochem. 2025 Mar 25;0(0):EBC20243000. doi: 10.1042/EBC20243000. Essays Biochem. 2025. PMID: 40134277 Free PMC article. Review.
-
GWAS for Defining the Pathogenesis of Hypertension: Have They Delivered?Hypertension. 2025 Apr;82(4):573-582. doi: 10.1161/HYPERTENSIONAHA.124.23451. Epub 2025 Feb 12. Hypertension. 2025. PMID: 39936322 Review.
-
The immune system in cardiovascular diseases: from basic mechanisms to therapeutic implications.Signal Transduct Target Ther. 2025 May 23;10(1):166. doi: 10.1038/s41392-025-02220-z. Signal Transduct Target Ther. 2025. PMID: 40404619 Free PMC article. Review.
-
Bone Marrow Niche in Cardiometabolic Disease: Mechanisms and Therapeutic Potential.Circ Res. 2025 Jan 31;136(3):325-353. doi: 10.1161/CIRCRESAHA.124.323778. Epub 2025 Jan 30. Circ Res. 2025. PMID: 39883790 Review.
References
-
- Collaborators, G. B. D. R. F. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 388, 1659–1724, doi:10.1016/S0140-6736(16)31679-8 (2016). - DOI - PMC - PubMed
-
- Whelton PK et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 138, e426–e483, doi:10.1161/CIR.0000000000000597 (2018). - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
