

Adaptive immune changes associate with clinical progression of Alzheimer's disease
- PMID: 38658964
- PMCID: PMC11044380
- DOI: 10.1186/s13024-024-00726-8
Adaptive immune changes associate with clinical progression of Alzheimer's disease
Abstract
Background: Alzheimer's disease (AD) is the most frequent cause of dementia. Recent evidence suggests the involvement of peripheral immune cells in the disease, but the underlying mechanisms remain unclear.
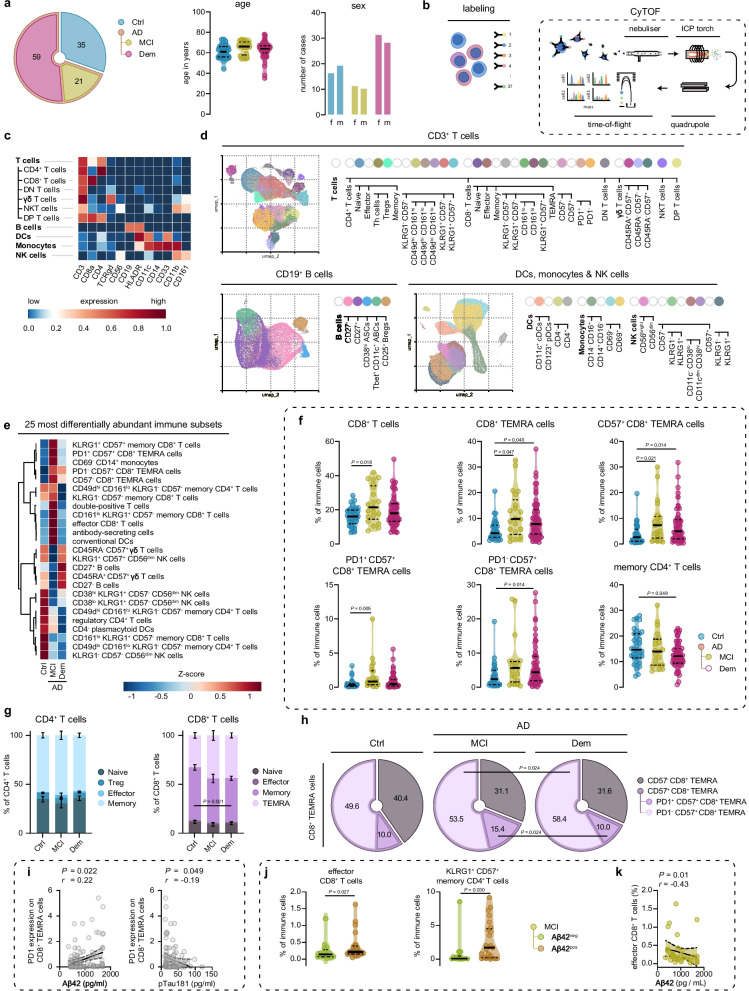
Methods: We comprehensively mapped peripheral immune changes in AD patients with mild cognitive impairment (MCI) or dementia compared to controls, using cytometry by time-of-flight (CyTOF).
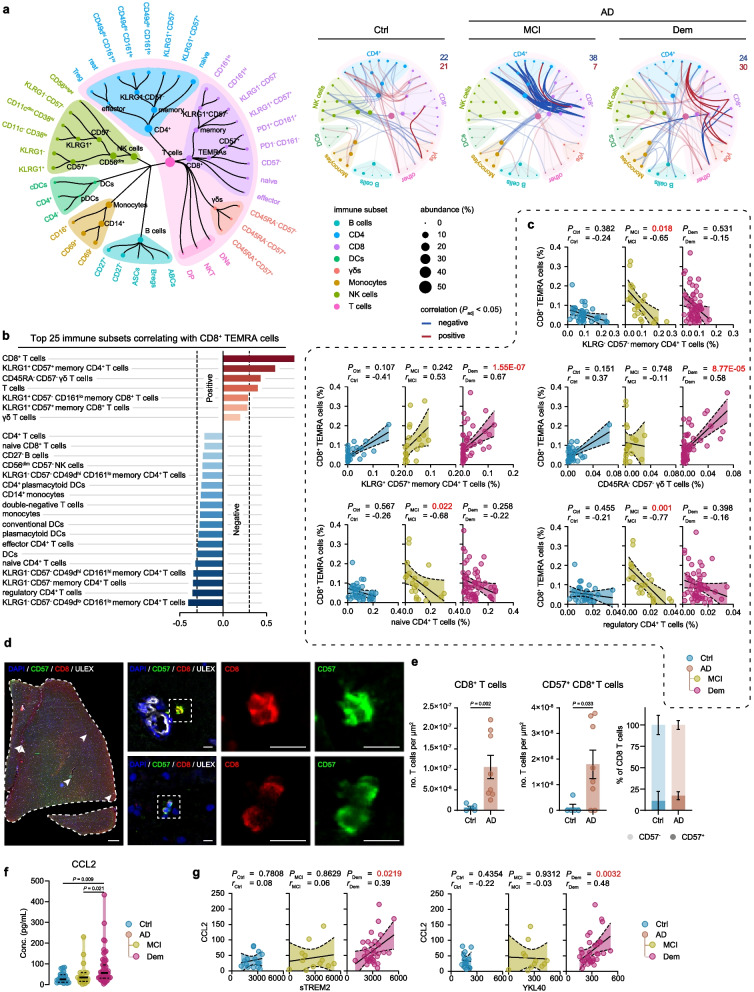
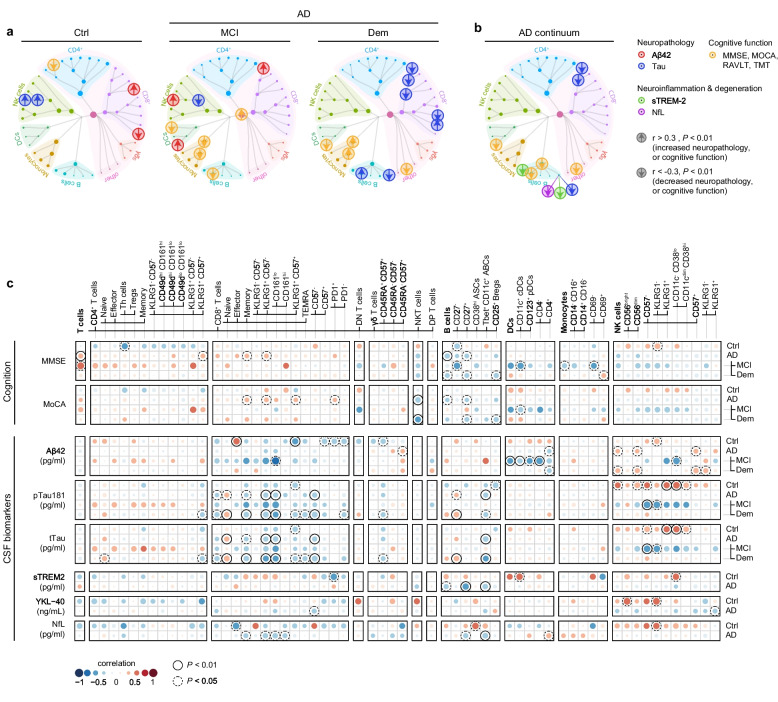
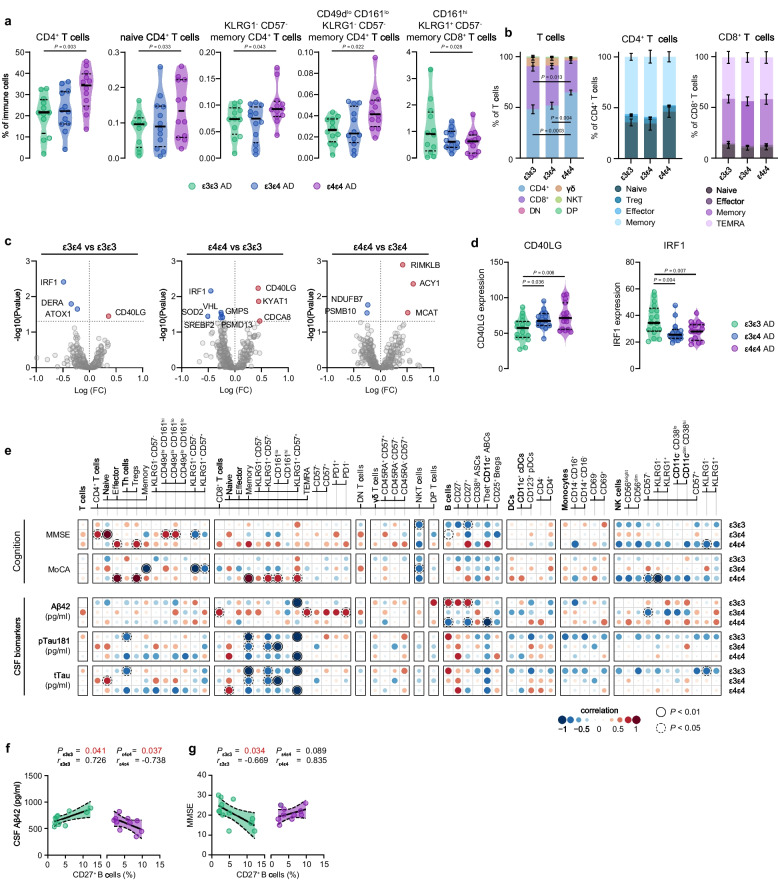
Results: We found an adaptive immune signature in AD, and specifically highlight the accumulation of PD1+ CD57+ CD8+ T effector memory cells re-expressing CD45RA in the MCI stage of AD. In addition, several innate and adaptive immune cell subsets correlated to cerebrospinal fluid (CSF) biomarkers of AD neuropathology and measures for cognitive decline. Intriguingly, subsets of memory T and B cells were negatively associated with CSF biomarkers for tau pathology, neurodegeneration and neuroinflammation in AD patients. Lastly, we established the influence of the APOE ε4 allele on peripheral immunity.
Conclusions: Our findings illustrate significant peripheral immune alterations associated with both early and late clinical stages of AD, emphasizing the necessity for further investigation into how these changes influence underlying brain pathology.
Keywords: APOE; Adaptive immunity; Alzheimer’s disease; Neuroinflammation; T cells; TEMRA cells.
© 2024. The Author(s).
Conflict of interest statement
CET has research contracts with Acumen, ADx Neurosciences, AC-Immune, Alamar, Aribio, Axon Neurosciences, Beckman-Coulter, BioConnect, Bioorchestra, Brainstorm Therapeutics, Celgene, Cognition Therapeutics, EIP Pharma, Eisai, Eli Lilly, Fujirebio, Instant Nano Biosensors, Novo Nordisk, Olink, PeopleBio, Quanterix, Roche, Toyama, Vivoryon. CET is editor in chief of Alzheimer Research and Therapy, and serves on editorial boards of Medidact Neurologie/Springer, and Neurology: Neuroimmunology & Neuroinflammation. CET had consultancy/speaker contracts for Eli Lilly, Merck, Novo Nordisk, Olink and Roche. WMF has performed contract research for Biogen MA Inc, and Boehringer Ingelheim. WMF has been an invited speaker at Boehringer Ingelheim, Biogen MA Inc, Danone, Eisai, WebMD Neurology (Medscape), and Springer Healthcare. WMF has been a consultant to Oxford Health Policy Forum CIC, Roche, and Biogen MA Inc. WMF participated in advisory boards of Biogen MA Inc and Roche. WMF was associate editor of Alzheimer, Research & Therapy in 2020/2021. WMF is associate editor at Brain.
Figures
References
-
- Montagne A, Nikolakopoulou AM, Huuskonen MT, Sagare AP, Lawson EJ, Lazic D, et al. APOE4 accelerates advanced-stage vascular and neurodegenerative disorder in old Alzheimer’s mice via cyclophilin A independently of amyloid-β. Nature Aging. 2021;1(6):506–520. doi: 10.1038/s43587-021-00073-z. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
