

Emergency physician resource utilization varies by years of experience
- PMID: 38659596
- PMCID: PMC11040178
- DOI: 10.1002/emp2.13162
Emergency physician resource utilization varies by years of experience
Abstract
Objectives: One of the most pivotal decisions an emergency physician (EP) makes is whether to admit or discharge a patient. The emergency department (ED) work-up leading to this decision involves several resource-intensive tests. Previous studies have demonstrated significant differences in EP resource utilization, measured by lab tests, advanced imaging (magnetic resonance imaging [MRI], computed tomography [CT], ultrasound), consultations, and propensity to admit a patient. However, how an EP's years of experience may impact their resource utilization and propensity to admit patients has not been well characterized. This study seeks to better understand how EPs' years of experience, post-residency, relates to their use of advanced imaging and patient disposition.
Methods: Ten years of ED visits were analyzed for this study from a single, academic tertiary care center in the urban Northeast United States. The primary outcomes were utilization of advanced imaging during the visit (CT, MRI, or formal ultrasound) and whether the patient was admitted. EP years of experience was categorized into 0-2 years, 3-5 years, 6-8 years, 9-11 years, and 12 or more years. Patient age, sex, Emergency Severity Index (ESI), and the attending EP's years of experience were collected. The relationship between EP years of experience and each outcome was assessed with a linear mixed model with a random effect for provider and patient age, sex, and ESI as covariates.
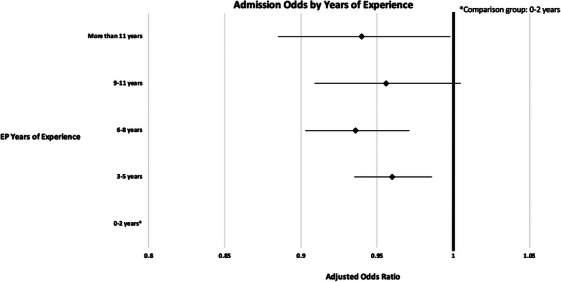
Results: A total of 460,937 visits seen by 65 EPs were included in the study. Over one-third (37.6%) of visits had an advanced imaging study ordered and nearly half (49.5%) resulted in admission. Compared to visits with EPs with 0-2 years of experience, visits with EPs with 3-5 or 6-8 years of experience had significantly lower odds of advanced imaging occurring. Visits seen by EPs with more than 2 years of experience had lower odds of admission than visits by EPs with 0-2 years of experience.
Conclusion: More junior EPs tend to order more advanced imaging studies and have a higher propensity to admit patients. This may be due to less comfort in decision-making without advanced imaging or a lower risk tolerance. Conversely, the additional clinical experience of the most senior EPs, with greater than 9 years of experience, likely impacts their resource utilization patterns such that their use of advanced imaging does not significantly differ from the most junior EPs.
Keywords: administration; length of stay; operations; quality; resource utilization; safety.
© 2024 The Authors. Journal of the American College of Emergency Physicians Open published by Wiley Periodicals LLC on behalf of American College of Emergency Physicians.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
LinkOut - more resources
Full Text Sources
Miscellaneous
