

This is a preprint.
Surgical Delay-Associated Mortality Risk Varies by Subtype in Loco-Regional Breast Cancer Patients in SEER-Medicare
- PMID: 38659868
- PMCID: PMC11042396
- DOI: 10.21203/rs.3.rs-4171651/v1
Surgical Delay-Associated Mortality Risk Varies by Subtype in Loco-Regional Breast Cancer Patients in SEER-Medicare
Update in
-
Surgical delay-associated mortality risk varies by subtype in loco-regional breast cancer patients in SEER-Medicare.Breast Cancer Res. 2024 Dec 30;26(1):191. doi: 10.1186/s13058-024-01949-9. Breast Cancer Res. 2024. PMID: 39736650 Free PMC article.
Abstract
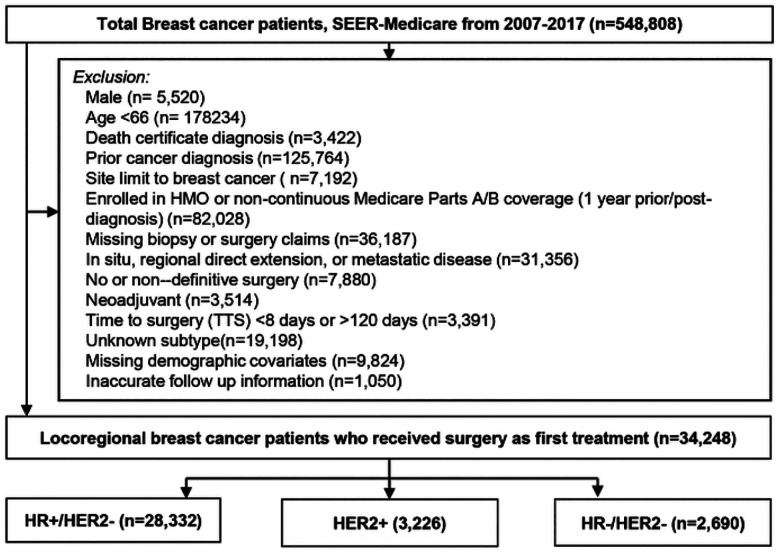
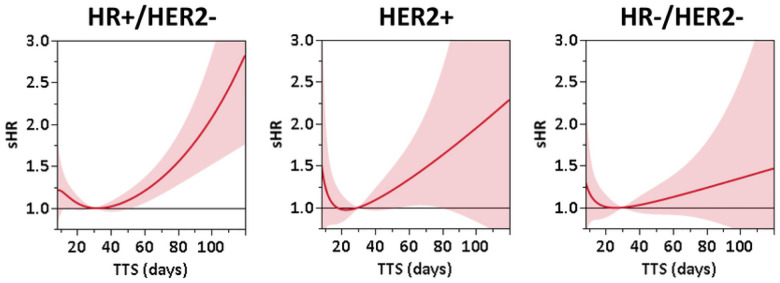
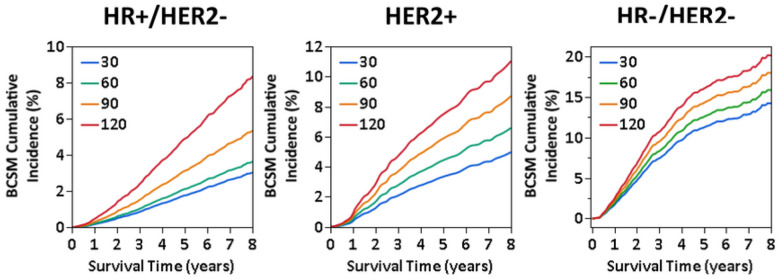
Substantial evidence supports that delay of surgery after breast cancer diagnosis is associated with increased mortality risk, leading to the introduction of a new Commission on Cancer quality measure for receipt of surgery within 60 days of diagnosis for non-neoadjuvant patients. Breast cancer subtype is a critical prognostic factor and determines treatment options; however, it remains unknown whether surgical delay-associated breast cancer-specific mortality (BCSM) risk differs by subtype. This retrospective cohort study aimed to assess whether the impact of delayed surgery on survival varies by subtype (hormone [HR]+/HER2-, HR-/HER2-, and HER2+) in patients with loco-regional breast cancer who received surgery as their first treatment between 2010-2017 using the SEER-Medicare. Continuous time to surgery from diagnostic biopsy (TTS; days) in reference to TTS = 30 days. BCSM were evaluated as flexibly dependent on continuous time (days) to surgery from diagnosis (TTS) using Cox proportional hazards and Fine and Gray competing-risk regression models, respectively, by HR status. Inverse propensity score-weighting was used to adjust for demographic, clinical, and treatment variables impacting TTS. Adjusted BCSM risk grew with increasing TTS across all subtypes, however, the pattern and extent of the association varied. HR+/HER2- patients exhibited the most pronounced increase in BCSM risk associated with TTS, with approximately exponential growth after 42 days, with adjusted subdistribution hazard ratios (sHR) of 1.21 (95% CI: 1.06-1.37) at TTS = 60 days, 1.79 (95% CI: 1.40-2.29) at TTS = 90 days, and 2.83 (95% CI: 1.76-4.55) at TTS = 120 days. In contrast, both HER2 + and HR-/HER2- patients showed slower, approximately linear growth in sHR, although non-significant in HR-HER2-.
Keywords: Breast cancer-specific mortality; HER2; Hormone-receptor; SEER-Medicare; Surgical delay; Tumor subtype.
Conflict of interest statement
Competing Interest: All authors declare no financial or non-financial competing interests.
Figures
References
-
- Eriksson L, Bergh J, Humphreys K, Warnberg F, Tornberg S, Czene K. Time from breast cancer diagnosis to therapeutic surgery and breast cancer prognosis: A population-based cohort study. Int J Cancer. 2018. - PubMed
-
- Shin DW, Cho J, Kim SY, et al. Delay to curative surgery greater than 12 weeks is associated with increased mortality in patients with colorectal and breast cancer but not lung or thyroid cancer. Ann Surg Oncol. 2013;20(8):2468–2476. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
