

Kidney involvement in Wilson's disease: a review of the literature
- PMID: 38660122
- PMCID: PMC11040517
- DOI: 10.1093/ckj/sfae058
Kidney involvement in Wilson's disease: a review of the literature
Abstract
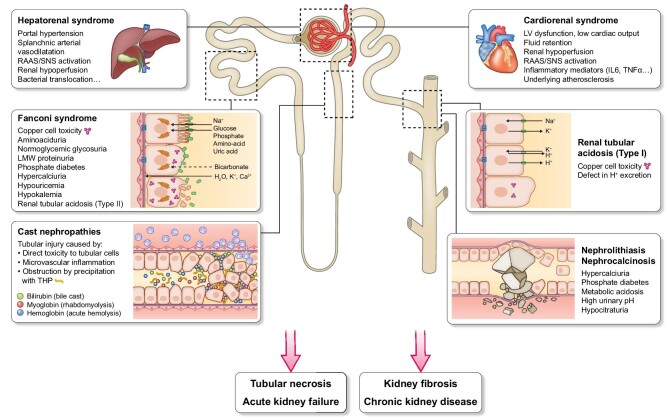
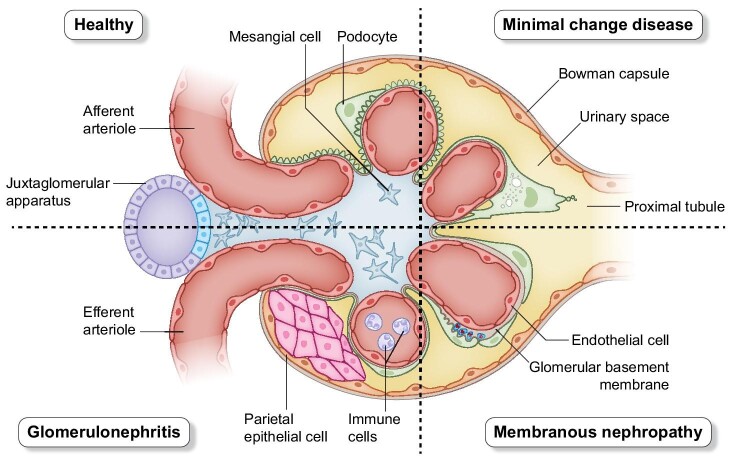
Wilson's disease (WD) is a rare inherited disease due to the mutation of the ATP7B gene, resulting in impaired hepatic copper excretion and its pathological accumulation in various organs such as the liver, the nervous system, or the kidneys. Whereas liver failure and neuropsychiatric disorders are the most common features, less is known about the renal complications. We conducted a review of the literature to define the characteristics and pathophysiology of kidney involvement during WD. This review shed light on strong evidence for direct copper toxicity to renal tubular cells. Excessive tubular copper accumulation might present with various degrees of tubular dysfunction, ranging from mild hydroelectrolytic and acid-base disorders to complete Fanconi syndrome. Proximal and distal renal tubular acidosis also favors development of nephrolithiasis, nephrocalcinosis, and bone metabolism abnormalities. Indirect complications might involve renal hypoperfusion as occurs in hepatorenal or cardiorenal syndrome, but also tubular casts' formation during acute hemolysis, rhabdomyolysis, or bile cast nephropathy. Acute kidney failure is not uncommon in severe WD patients, and independently increases mortality. Finally, specific and long-term therapy by D-penicillamin, one of the most efficient drugs in WD, can cause glomerular injuries, such as membranous nephropathy, minimal-change disease, and, rarely, severe glomerulonephritis. Altogether, our study supports the need for interdisciplinary evaluation of WD patients involving nephrologists, with regular monitoring of tubular and glomerular functions, to provide adequate prevention of renal and bone involvement.
Keywords: Fanconi syndrome; Wilson's disease; hypercalciuria; nephrolithiasis; renal acidosis.
© The Author(s) 2024. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
None declared.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
