

Liver regeneration after portal and hepatic vein embolization improves overall survival compared with portal vein embolization alone: mid-term survival analysis of the multicentre DRAGON 0 cohort
- PMID: 38662462
- PMCID: PMC11044894
- DOI: 10.1093/bjs/znae087
Liver regeneration after portal and hepatic vein embolization improves overall survival compared with portal vein embolization alone: mid-term survival analysis of the multicentre DRAGON 0 cohort
Abstract
Background: The purpose of this study was to compare 3-year overall survival after simultaneous portal (PVE) and hepatic vein (HVE) embolization versus PVE alone in patients undergoing liver resection for primary and secondary cancers of the liver.
Methods: In this multicentre retrospective study, all DRAGON 0 centres provided 3-year follow-up data for all patients who had PVE/HVE or PVE, and were included in DRAGON 0 between 2016 and 2019. Kaplan-Meier analysis was undertaken to assess 3-year overall and recurrence/progression-free survival. Factors affecting survival were evaluated using univariable and multivariable Cox regression analyses.
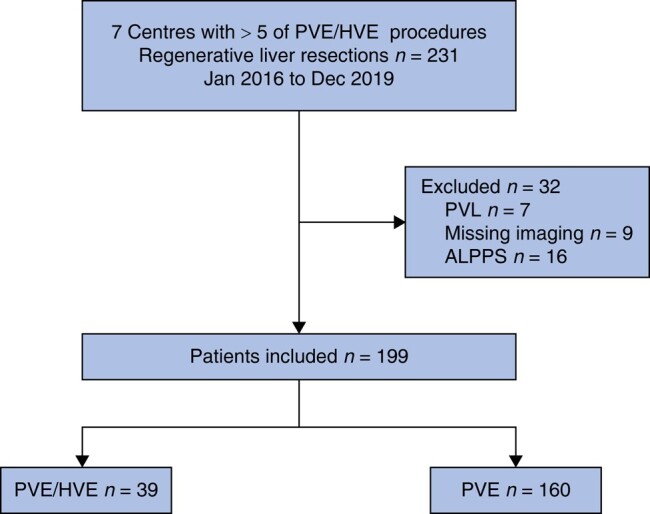
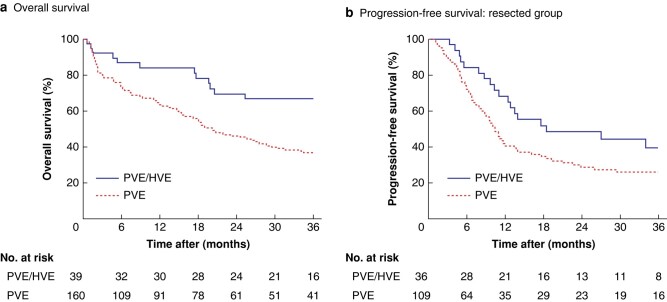
Results: In total, 199 patients were included from 7 centres, of whom 39 underwent PVE/HVE and 160 PVE alone. Groups differed in median age (P = 0.008). As reported previously, PVE/HVE resulted in a significantly higher resection rate than PVE alone (92 versus 68%; P = 0.007). Three-year overall survival was significantly higher in the PVE/HVE group (median survival not reached after 36 months versus 20 months after PVE; P = 0.004). Univariable and multivariable analyses identified PVE/HVE as an independent predictor of survival (univariable HR 0.46, 95% c.i. 0.27 to 0.76; P = 0.003).
Conclusion: Overall survival after PVE/HVE is substantially longer than that after PVE alone in patients with primary and secondary liver tumours.
© The Author(s) 2024. Published by Oxford University Press on behalf of BJS Foundation Ltd.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
