

Cervical spine immobilisation following blunt trauma in pre-hospital and emergency care: A systematic review
- PMID: 38662734
- PMCID: PMC11045128
- DOI: 10.1371/journal.pone.0302127
Cervical spine immobilisation following blunt trauma in pre-hospital and emergency care: A systematic review
Abstract
Objectives: To assess whether different cervical spine immobilisation strategies (full immobilisation, movement minimisation or no immobilisation), impact neurological and/or other outcomes for patients with suspected cervical spinal injury in the pre-hospital and emergency department setting.
Design: Systematic review following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Data sources: MEDLINE, EMBASE, CINAHL, Cochrane Library and two research registers were searched until September 2023.
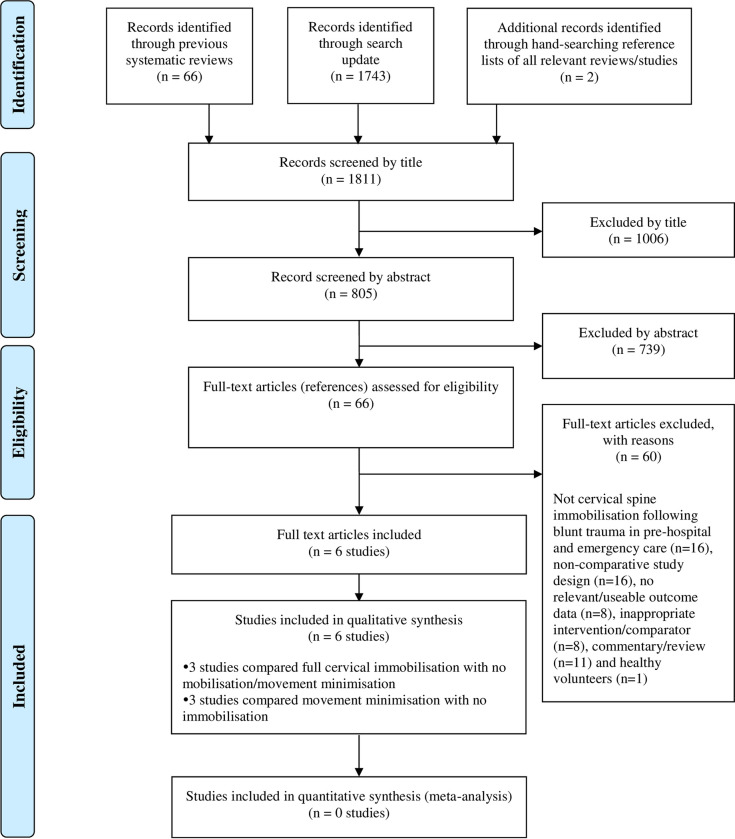
Eligibility criteria: All comparative studies (prospective or retrospective) that examined the potential benefits and/or harms of immobilisation practices during pre-hospital and emergency care of patients with a potential cervical spine injury (pre-imaging) following blunt trauma.
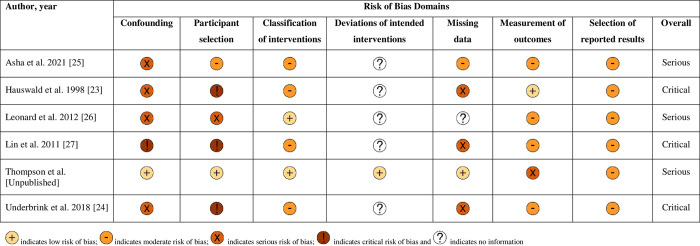
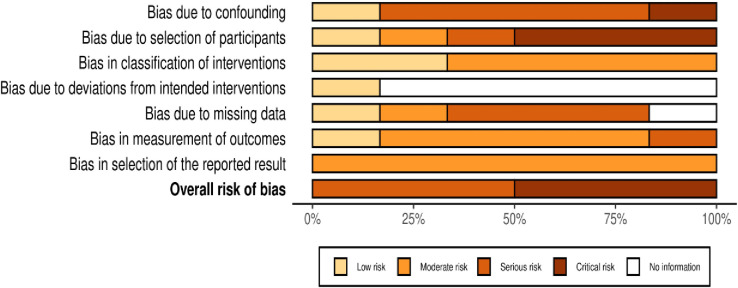
Data extraction and synthesis: Two authors independently selected and extracted data. Risk of bias was appraised using the Cochrane ROBINS-I tool for non-randomised studies. Data were synthesised without meta-analysis.
Results: Six observational studies met the inclusion criteria. The methodological quality was variable, with most studies having serious or critical risk of bias. The effect of cervical spine immobilisation practices such as full immobilisation or movement minimisation during pre-hospital and emergency care did not show clear evidence of benefit for the prevention of neurological deterioration, spinal injuries and death compared with no immobilisation. However, increased pain, discomfort and anatomical complications were associated with collar application during immobilisation.
Conclusions: Despite the limited evidence, weak designs and limited generalisability, the available data suggest that pre-hospital cervical spine immobilisation (full immobilisation or movement minimisation) was of uncertain value due to the lack of demonstrable benefit and may lead to potential complications and adverse outcomes. High-quality randomised comparative studies are required to address this important question.
Trial registration: PROSPERO REGISTRATION Fiona Lecky, Abdullah Pandor, Munira Essat, Anthea Sutton, Carl Marincowitz, Gordon Fuller, Stuart Reid, Jason Smith. A systematic review of cervical spine immobilisation following blunt trauma in pre-hospital and emergency care. PROSPERO 2022 CRD42022349600 Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022349600.
Copyright: © 2024 Pandor et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
All authors declare grant funding to their employing institutions from the United Kingdom National Institute for Health and Care Research (NIHR) Health Technology Assessment (HTA) Programme, as outlined in the funding statement. These competing interests do not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- National Clinical Guideline Centre (UK). Spinal Injury: Assessment and Initial Management (NG41): London: National Institute for Health and Care Excellence (NICE); 2016. Available from: https://www.nice.org.uk/guidance/ng41/evidence/full-guideline-2358425776. - PubMed
-
- American College of Surgeons. ATLS—Advanced Trauma Life Support: Student Course Manual 10th Edition: Chicago; American College of Surgeons.; 2018. Available from: https://www.emergencymedicinekenya.org/wp-content/uploads/2021/09/ATLS-1....
-
- Kornhall DK, Jorgensen JJ, Brommeland T, Hyldmo PK, Asbjornsen H, Dolven T, et al.. The Norwegian guidelines for the prehospital management of adult trauma patients with potential spinal injury. Scandinavian Journal of Trauma, Resuscitation & Emergency Medicine. 2017;25(1):2. doi: 10.1186/s13049-016-0345-x - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
