

Proteomics, Human Environmental Exposure, and Cardiometabolic Risk
- PMID: 38662804
- PMCID: PMC11189739
- DOI: 10.1161/CIRCRESAHA.124.324559
Proteomics, Human Environmental Exposure, and Cardiometabolic Risk
Abstract
Background: The biological mechanisms linking environmental exposures with cardiovascular disease pathobiology are incompletely understood. We sought to identify circulating proteomic signatures of environmental exposures and examine their associations with cardiometabolic and respiratory disease in observational cohort studies.
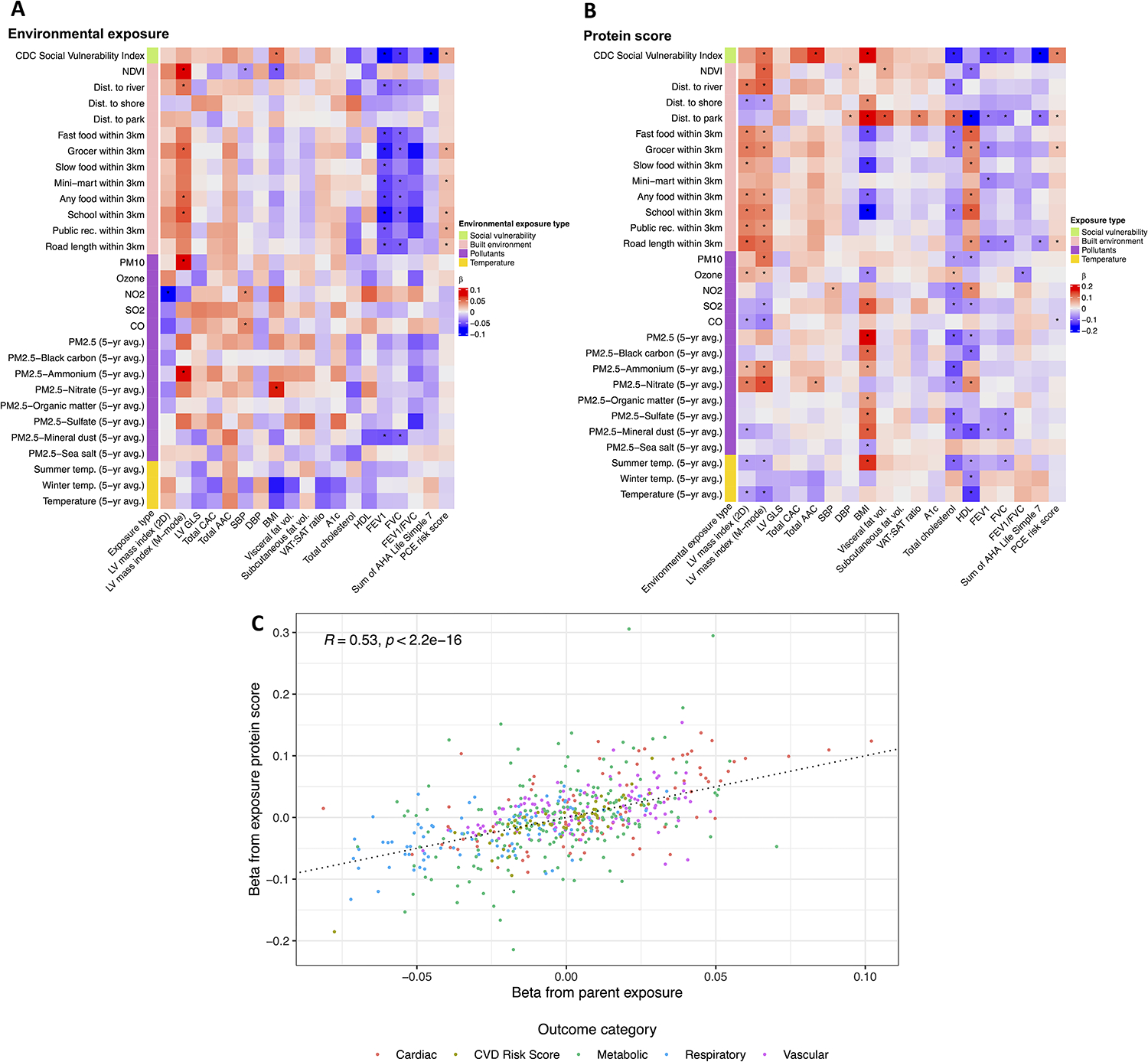
Methods: We tested the relations of >6500 circulating proteins with 29 environmental exposures across the built environment, green space, air pollution, temperature, and social vulnerability indicators in ≈3000 participants of the CARDIA study (Coronary Artery Risk Development in Young Adults) across 4 centers using penalized and ordinary linear regression. In >3500 participants from FHS (Framingham Heart Study) and JHS (Jackson Heart Study), we evaluated the prospective relations of proteomic signatures of the envirome with cardiovascular disease and mortality using Cox models.
Results: Proteomic signatures of the envirome identified novel/established cardiovascular disease-relevant pathways including DNA damage, fibrosis, inflammation, and mitochondrial function. The proteomic signatures of the envirome were broadly related to cardiometabolic disease and respiratory phenotypes (eg, body mass index, lipids, and left ventricular mass) in CARDIA, with replication in FHS/JHS. A proteomic signature of social vulnerability was associated with a composite of cardiovascular disease/mortality (1428 events; FHS: hazard ratio, 1.16 [95% CI, 1.08-1.24]; P=1.77×10-5; JHS: hazard ratio, 1.25 [95% CI, 1.14-1.38]; P=6.38×10-6; hazard ratio expressed as per 1 SD increase in proteomic signature), robust to adjustment for known clinical risk factors.
Conclusions: Environmental exposures are related to an inflammatory-metabolic proteome, which identifies individuals with cardiometabolic disease and respiratory phenotypes and outcomes. Future work examining the dynamic impact of the environment on human cardiometabolic health is warranted.
Keywords: cardiovascular diseases; environment; heart failure; hypertension; myocardial infarction; risk factors.
Conflict of interest statement
Figures





References
-
- Li F, Harmer P, Cardinal BJ, Bosworth M, Johnson-Shelton D, Moore JM, Acock A, Vongjaturapat N. Built environment and 1-year change in weight and waist circumference in middle-aged and older adults: Portland Neighborhood Environment and Health Study. Am J Epidemiol. 2009;169:401–408. doi: 10.1093/aje/kwn398 - DOI - PMC - PubMed
-
- Bhatnagar A Environmental cardiology: studying mechanistic links between pollution and heart disease. Circ Res. 2006;99:692–705. doi: 10.1161/01.RES.0000243586.99701.cf - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
