

Radiation Therapy With or Without Cisplatin for Local Recurrences of Endometrial Cancer: Results From an NRG Oncology/GOG Prospective Randomized Multicenter Clinical Trial
- PMID: 38662968
- PMCID: PMC11681946
- DOI: 10.1200/JCO.23.01279
Radiation Therapy With or Without Cisplatin for Local Recurrences of Endometrial Cancer: Results From an NRG Oncology/GOG Prospective Randomized Multicenter Clinical Trial
Abstract
Purpose: Pelvic recurrence is a frequent pattern of relapse for women with endometrial cancer. A randomized trial compared progression-free survival (PFS) after treatment with radiation therapy alone as compared with concurrent chemotherapy.
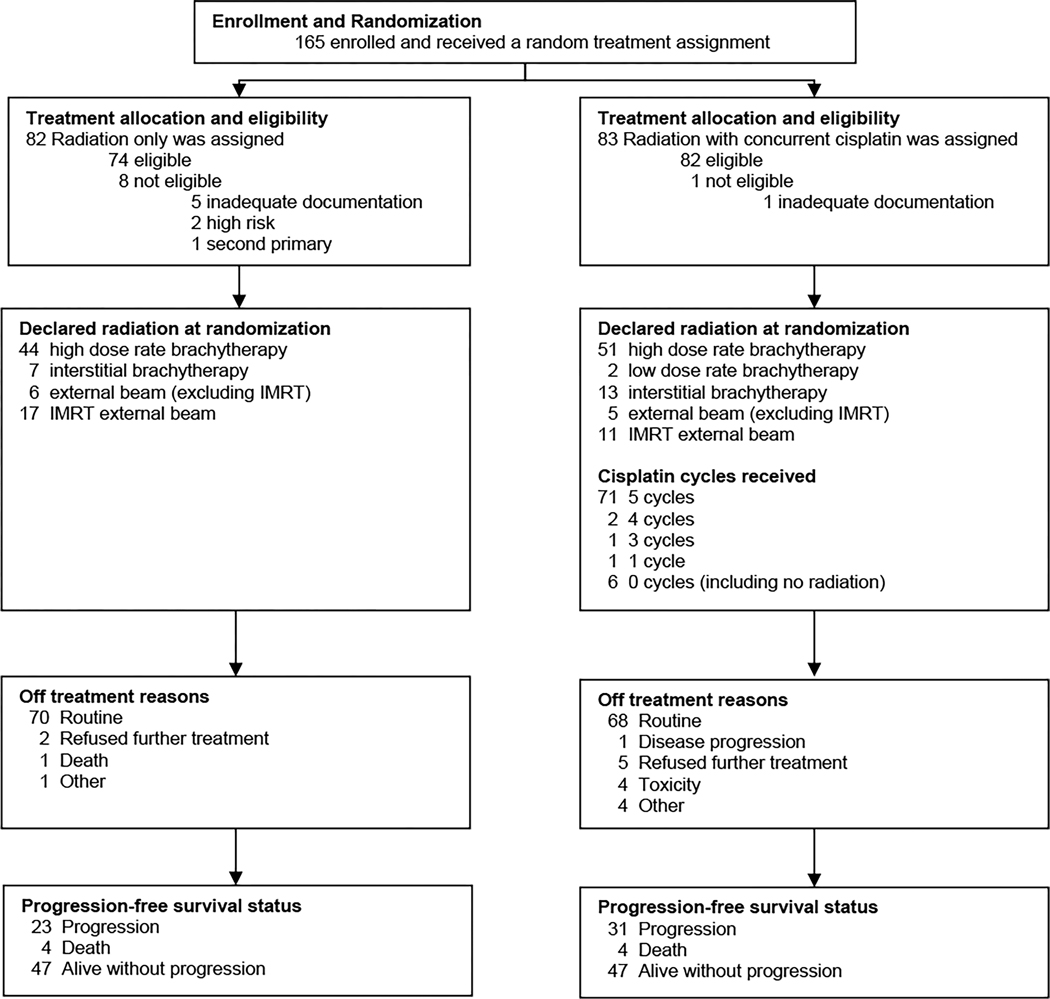
Materials and methods: Between February 2008 and August 2020, 165 patients were randomly assigned 1:1 to receive either radiation treatment alone or a combination of chemotherapy and radiation treatment. The primary objective of this study was to determine whether chemoradiation therapy was more effective than radiation therapy alone at improving PFS.
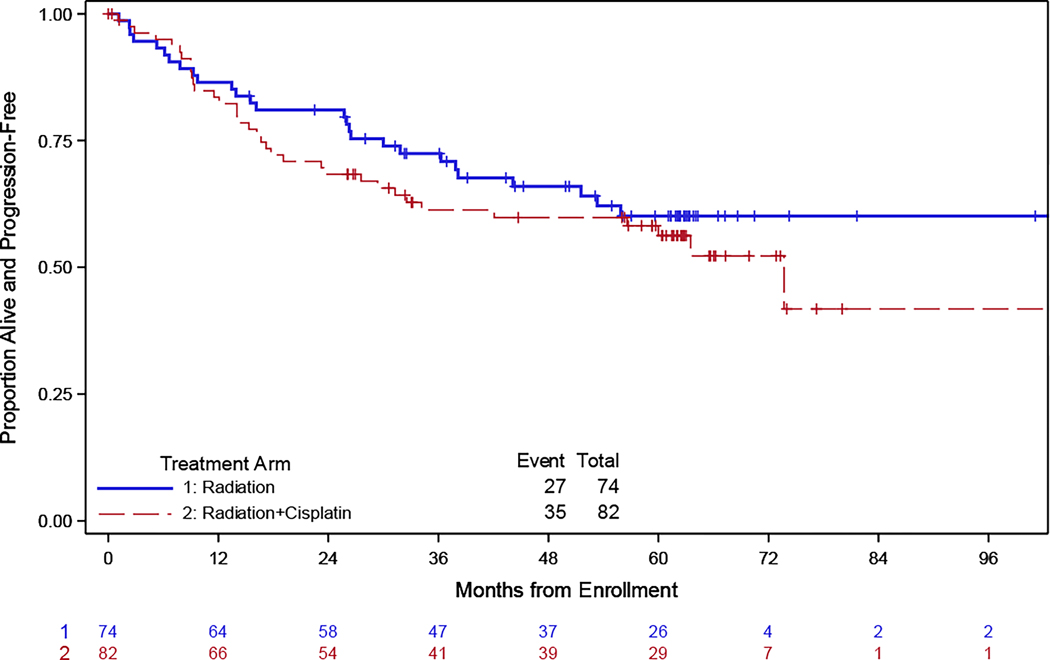
Results: The majority of patients had low-grade (1 or 2) endometrioid histology (82%) and recurrences confined to the vagina (86%). External beam with either the three-dimensional or intensity modulated radiation treatment technique was followed by a boost delivered with brachytherapy or external beam. Patients randomly assigned to receive chemotherapy were treated with once weekly cisplatin (40 mg/m2). Rates of acute toxicity were higher in patients treated with chemoradiation as compared with radiation treatment alone. Median PFS was longer for patients treated with radiation therapy alone as compared with chemotherapy and radiation (median PFS was not reached for RT v 73 months for chemoradiation, hazard ratio of 1.25 (95% CI, 0.75 to 2.07). At 3 years, 73% of patients treated definitively with radiation and 62% of patients treated with chemoradiation were alive and free of disease progression.
Conclusion: Excellent outcomes can be achieved for women with localized recurrences of endometrial cancer when treated with radiation therapy. The addition of chemotherapy does not improve PFS for patients treated with definitive radiation therapy for recurrent endometrial cancer and increases acute toxicity. Patients with low-grade and vaginal recurrences who constituted the majority of those enrolled are best treated with radiation therapy alone.
Conflict of interest statement
The following authors have no conflicts of interest to disclose: Dr. Ann Klopp, Dr. Susan Zweizig, Dr. Steven Waggoner, Dr. Lana de Souza Lawrence, Dr. Parviz Hanjani, Dr. Higinia Cardenes, Dr. William Small and Dr. Jonathan Feddock.
Dr. Danielle Enserro wishes to disclose that NCI support was received as Cooperative Grant/NCTN Grant funding for all aspects of this trial including travel to group meetings, statistical analysis, study monitoring, etc.
Dr. Matthew Powell acknowledges receiving consulting fees from the following: GlaxoSmithKline GSK/Tesaro, Merck, AstraZeneca, Clovis Oncology, Seagen and Eisai.
Dr. Marcus Randall reports receiving support for attending GOG/NRG travel and meeting support as Co-Chair of the Uterine Corpus Committee.
Dr. Robert Mannel and Dr. Laura Holman report institutional support received from NCI clinical trials network in support of this manuscript.
Dr. David Bender has received grants from Tesaro, Inc., AbbVie, Inc., AstraZeneca, Merck Sharp & Dohme Company, Clovis Oncology, Inc. and Genentech.
Dr. Christina Kushnir received consulting fees from Intuitive Surgical and Ethicon Biosurgery.
Dr. Floor Backes acknowledges research grants to Institution from Merck, Eisai, Immunogen, Clovis, BeiGene, Natera and Tempus. Dr. Backes received personal fees from UptoDate. Additionally, Dr. Backes received consulting fees from Agenus, Merck, Clovis, Immunogen, Eisai, AstraZeneca, GlaxoSmithKline, Myriad and Genentech. Dr. Backes also received personal fees for CME lectures from Clinical Educational Concepts, Clinical Care Options, Medscape/WebMD, Med Learning, 13Health, CMR Institute, Global Learning Initiative/Prova, OncLive. Dr. Backes served as a Board Member for the Society of Gynecologic Oncology (unpaid), Co-Chair for both NRG Oncology Developmental Therapeutics Committee and IGCS Education360.
Dr. Kristin Bradley reports serving as Treasurer of the American Brachytherapy Society (unpaid position) and is on the Board of Directors for the same.
Dr. Christopher Darus reports serving on the AstraZeneca Advisory Board and has received payments for the same. He also reports owning stock in Regeneron and Humanigen.
Dr. David Miller reports serving as Chair, Uterine Corpus Committee for GOG then NRG Oncology, 2003-2018.
Figures



References
-
- Siegel RL, Miller KD, Wagle NS & Jemal A. Cancer statistics, 2023. CA Cancer J Clin 73, 17–48 (2023). - PubMed
-
- Keys HM, et al. A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: a Gynecologic Oncology Group study. Gynecol Oncol 92, 744–751 (2004). - PubMed
-
- Creutzberg CL, et al. Survival after relapse in patients with endometrial cancer: results from a randomized trial. Gynecol Oncol 89, 201–209 (2003). - PubMed
-
- Creutzberg CL, et al. Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: multicentre randomised trial. PORTEC Study Group. Post Operative Radiation Therapy in Endometrial Carcinoma. Lancet 355, 1404–1411 (2000). - PubMed
-
- Jhingran A, Burke TW & Eifel PJ Definitive radiotherapy for patients with isolated vaginal recurrence of endometrial carcinoma after hysterectomy. Int J Radiat Oncol Biol Phys 56, 1366–1372 (2003). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
