

Risk stratification refinements with inclusion of haemodynamic variables at follow-up in patients with pulmonary arterial hypertension
- PMID: 38663975
- PMCID: PMC11375514
- DOI: 10.1183/13993003.00197-2024
Risk stratification refinements with inclusion of haemodynamic variables at follow-up in patients with pulmonary arterial hypertension
Abstract
Background: Haemodynamic variables are prognostic factors in pulmonary arterial hypertension (PAH). However, right heart catheterisation (RHC) is not systematically recommended to assess the risk status during follow-up. This study aimed to assess the added value of haemodynamic variables in prevalent patients to predict the risk of death or lung transplantation according to their risk status assessed by the non-invasive four-strata model as recommended by the European guidelines.
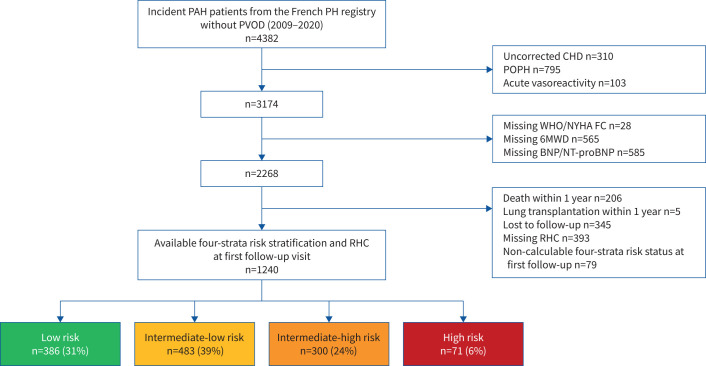
Methods: We evaluated incident patients with PAH enrolled in the French pulmonary hypertension registry between 2009 and 2020 who had a first follow-up RHC. Cox regression identified, in each follow-up risk status, haemodynamic variables significantly associated with transplant-free survival. Optimal thresholds were determined by time-dependent receiver operating characteristics. Several multivariable Cox regression models were performed to identify the haemodynamic variables improving the non-invasive risk stratification model.
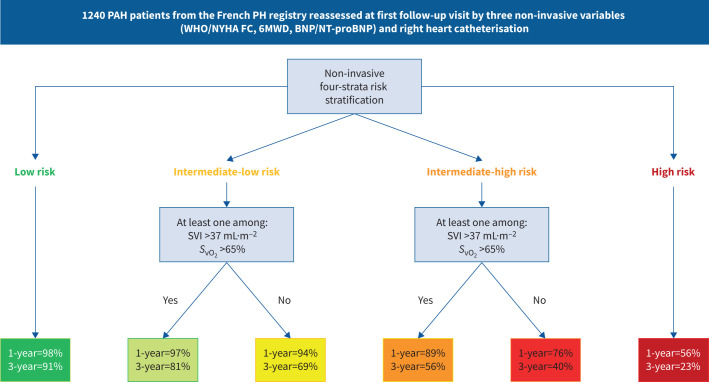
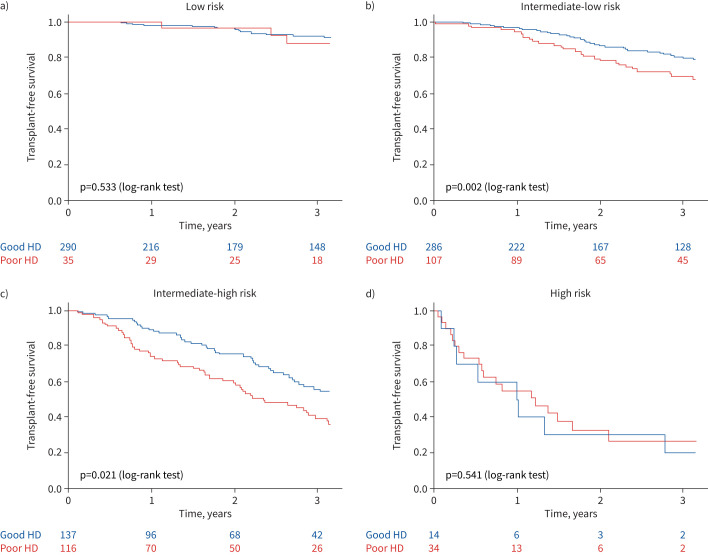
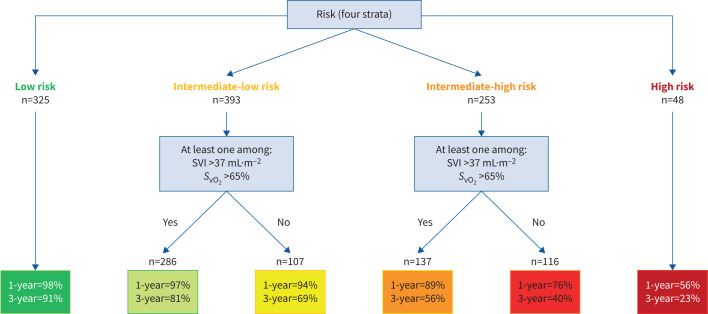
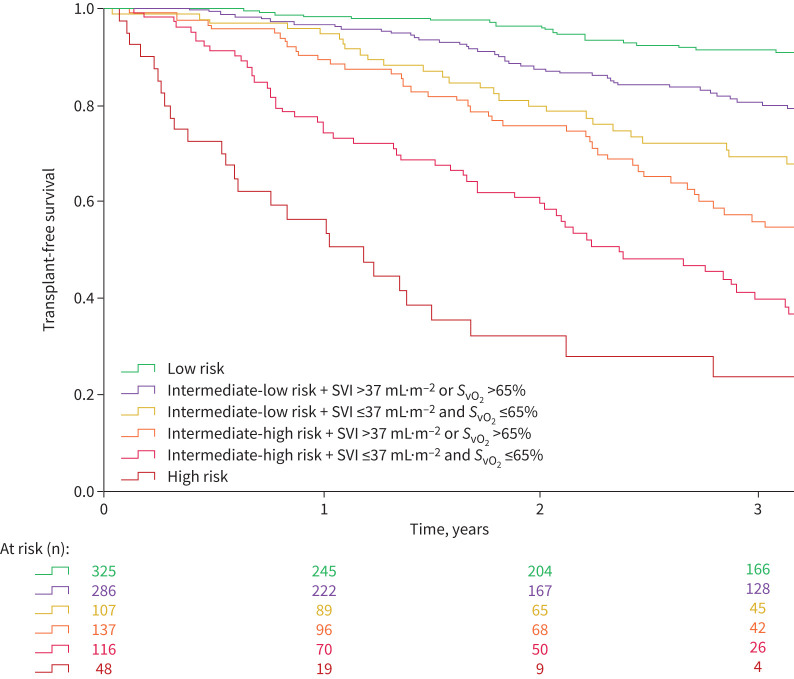
Results: We analysed 1240 incident patients reassessed within 1 year by RHC. None of the haemodynamic variables were significantly associated with transplant-free survival among low-risk (n=386) or high-risk (n=71) patients. Among patients at intermediate (intermediate-low, n=483 and intermediate-high, n=300) risk at first follow-up, multivariable models including either stroke volume index (SVI) or mixed venous oxygen saturation (S vO2 ) were the best. The prognostic performance of a refined six-strata risk stratification model including the non-invasive four-strata model and SVI >37 mL·m-2 and/or S vO2 >65% for patients at intermediate risk (area under the curve (AUC) 0.81; c-index 0.74) was better than that of the four-strata model (AUC 0.79, p=0.009; c-index 0.72).
Conclusion: Cardiopulmonary haemodynamics may improve risk stratification at follow-up in patients at intermediate risk.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: A. Boucly reports grants from Acceleron, Janssen and MSD, and lecture honoraria and travel support from Janssen, Merck, AOP Orphan and Ferrer, outside the submitted work. S. Turquier reports consulting fees from Ferrer, lecture honoraria from MSD, and travel support from Ferrer, MSD and Janssen, outside the submitted work. P. de Groote reports consulting fees from Boehringer Ingelheim, Servier, Bayer and MSD, and lecture honoraria from BMS, Novartis, Vifor and Pfizer, outside the submitted work. A. Chaouat reports travel support from MSD and Janssen, outside the submitted work. C. Cheron reports travel support from MSD, outside the submitted work. X. Jaïs reports grants from Acceleron, Janssen, MSD and Bayer HealthCare, and lecture honoraria from Janssen and MSD, outside the submitted work. F. Picard reports lecture honoraria from Bayer, Boehringer Ingelheim/Lilly, Novartis, MSD, AstraZeneca and Novo Nordisk, and travel support from Bayer and Novartis, outside the submitted work. G. Prévot reports lecture honoraria and travel support from Janssen and MSD, outside the submitted work. V. Cottin reports consulting fees from Ferrer/United Therapeutics and Liquidia, and lecture honoraria from Ferrer/United Therapeutics, outside the submitted work. D. Montani reports grants from Acceleron, Merck MSD and Janssen, consulting fees from Acceleron, Merck MSD, Janssen and Ferrer; and lecture honoraria from Bayer, Janssen, Boehringer, Chiesi, GSK, Ferrer and Merck MSD, outside the submitted work. M. Humbert reports grants from Acceleron, AOP Orphan, Janssen, Merck and Shou Ti, consulting fees from 35 Pharma, Aerovate, AOP Orphan, Bayer, Chiesi, Ferrer, Janssen, Keros, Merck, MorphogenIX, Shou Ti and United Therapeutics, lecture honoraria from Janssen and Merck, and advisory board participation with Acceleron, Altavant, Janssen, Merck and United Therapeutics, outside the submitted work. L. Savale reports lecture honoraria and travel support from MSD and Janssen and Janssen, outside the submitted work. O. Sitbon reports grants from Aerovate, AOP Orphan, Ferrer, Janssen and MSD, consulting fees from Altavant/Enzyvant, AOP Orphan, Ferrer, Gossamer Bio, Janssen, Liquidia, MSD and Respira Therapeutics, lecture honoraria from AOP Orphan, Janssen, Ferrer and MSD, and advisory board participation with Altavant/Enzyvant, Gossamer Bio and Janssen, outside the submitted work. The remaining authors have no potential conflicts of interest to disclose.
Figures
Comment in
-
The evolution of the European risk stratification system for pulmonary arterial hypertension.Eur Respir J. 2024 Sep 5;64(3):2400943. doi: 10.1183/13993003.00943-2024. Print 2024 Sep. Eur Respir J. 2024. PMID: 39237314 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources