

Interactive exploration of adverse events and multimorbidity in CKD
- PMID: 38664006
- PMCID: PMC11596092
- DOI: 10.1093/ndt/gfae092
Interactive exploration of adverse events and multimorbidity in CKD
Abstract
Background: Persons with chronic kidney disease (CKD) are at increased risk of adverse events, early mortality and multimorbidity. A detailed overview of adverse event types and rates from a large CKD cohort under regular nephrological care is missing. We generated an interactive tool to enable exploration of adverse events and their combinations in the prospective, observational German CKD (GCKD) study.
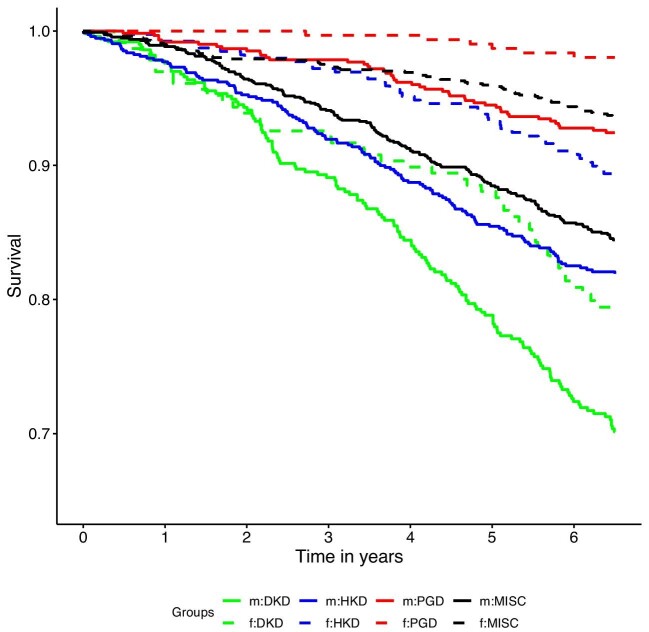
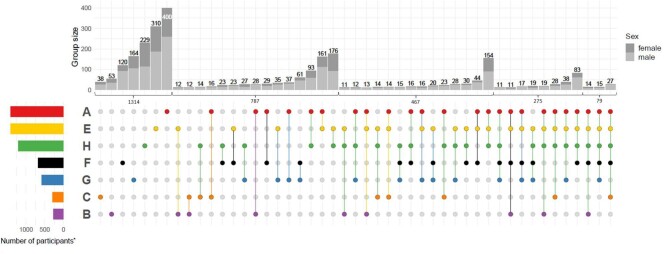
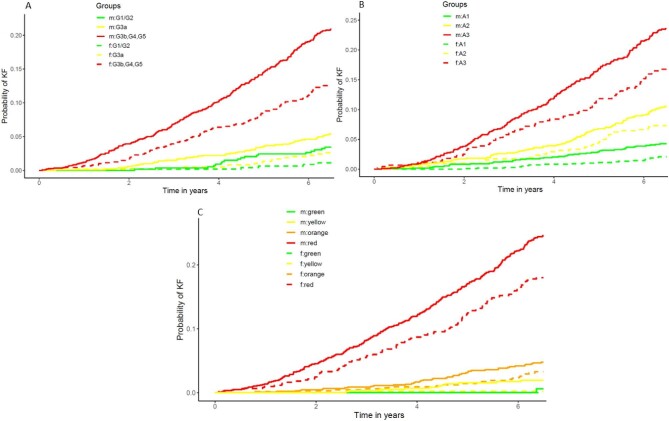
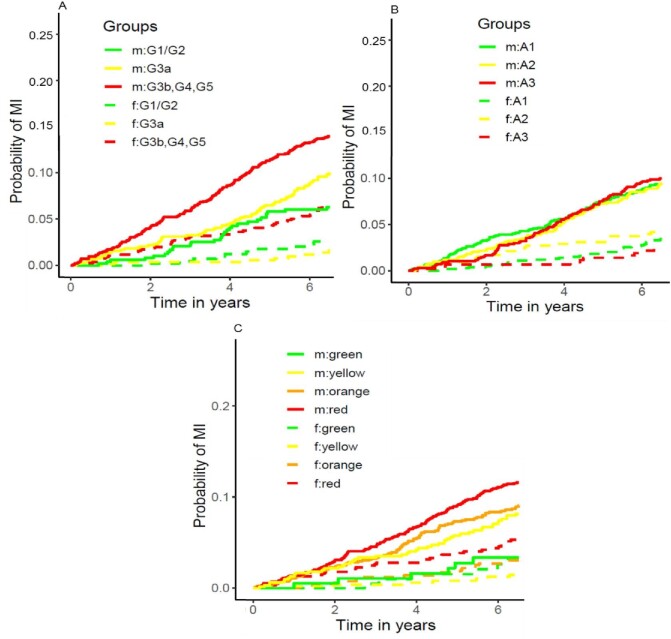
Methods: The GCKD study enrolled 5217 participants under regular nephrological care with an estimated glomerular filtration rate of 30-60 or >60 mL/min/1.73 m2 and an overt proteinuria. Cardiovascular, cerebrovascular and peripheral vascular, kidney, infection, and cancer events, as well as deaths were adjudicated following a standard operation procedure. We summarized these time-to-event data points for exploration in interactive graphs within an R shiny app. Multivariable adjusted Cox models for time to first event were fitted. Cumulative incidence functions, Kaplan-Meier curves and intersection plots were used to display main adverse events and their combinations by sex and CKD etiology.
Results: Over a median of 6.5 years, 10 271 events occurred in 2947 participants (56.5%), of which 680 participants (13.0%) died. The new publicly available interactive platform enables readers to scrutinize adverse events and their combinations as well as mortality trends as a gateway to better understand multimorbidity in CKD: incident rates per 1000 patient-years varied by event type, CKD etiology and baseline characteristics. Incidence rates for the most frequent events and their recurrence were 113.6 (cardiovascular), 75.0 (kidney) and 66.0 (infection). Participants with presumed diabetic kidney disease and men were more prone to experiencing events.
Conclusion: This comprehensive explorative tool to visualize adverse events (https://www.gckd.org/studienhintergrund/previous-study-results/event-analysis/), their combination, mortality and multimorbidity among persons with CKD may serve as a valuable resourec for patient care, identification of high-risk groups, health services and public health policy planning.
Keywords: adverse events; chronic kidney disease; epidemiology; interactive visualization; multimorbidity.
© The Author(s) 2024. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
The following conflict of interest statement is taken from the indication in the conflict of interest forms of each co-author. E.S. received consulting fees from AstraZeneca, honoraria, as a speaker from the National Kidney Foundation, is a board member of German Society of Nephrology and a KDIGO Working group. J.T.K. is stockholder with Synlab, BAYER and Quanterix Inc. J.F. received consulting fees and honoraria as a speaker from AstraZeneca, BAYER, Boehringer, CSL Vifor, Stadapharm, and Travere. C.W. received research grants for the institution from Boehringer Ingelheim, Sanofi and consulting fees from Amgen, Amicus, Astellas, AstraZeneca, BAYER, Boehringer Ingelheim, CSL Vifor, Chiesi, Chugai, Fresenius Medical Care, GSK, Idorsia, Eli Lilly, MSD, Novartis, Novo Nordisk, and Sanofi. A.K. received grant funding by the German Research Foundation (DFG) project ID 431984000 (SFB 1453) for the Institute of Genetic Epidemiology Freiburg. M.B. received consulting fees from Vifor Renal Pharma, Boehringer Ingelheim and honoraria as a speaker from AstraZeneca, Boehringer Ingelheim, Pfizer, Novartis Pharma, support for meeting registration/travel from Alexion Pharma. K.U.E. received grant funding from Evotec, Travere, AstraZeneca, consulting fees from Akebia, AstraZeneca, BAYER, Otsuka, Retrophin. J.M. received honoraria as a speaker from AstraZeneca, Boehringer Ingelheim, BAYER, Alexion, Lilly. The remaining authors disclosed no conflicts of interest.
Figures
References
-
- KDIGO clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 2013;3:1–150. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
