Subgroup analyses from the phase 3 ASCENT study of sacituzumab govitecan in metastatic triple-negative breast cancer
- PMID: 38664404
- PMCID: PMC11045722
- DOI: 10.1038/s41523-024-00635-5
Subgroup analyses from the phase 3 ASCENT study of sacituzumab govitecan in metastatic triple-negative breast cancer
Erratum in
-
Author Correction: Subgroup analyses from the phase 3 ASCENT study of sacituzumab govitecan in metastatic triple-negative breast cancer.NPJ Breast Cancer. 2024 Jul 9;10(1):55. doi: 10.1038/s41523-024-00666-y. NPJ Breast Cancer. 2024. PMID: 38982075 Free PMC article. No abstract available.
Abstract
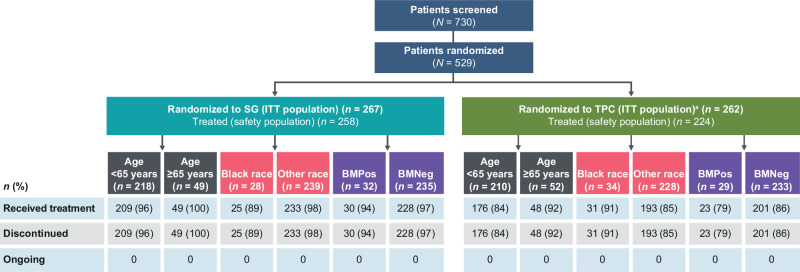
In this post hoc analysis of the ASCENT study, we compared outcomes with sacituzumab govitecan (SG) vs single-agent chemotherapy in clinically important subgroups of patients with metastatic triple-negative breast cancer (mTNBC). Patients with mTNBC refractory to/relapsing after ≥2 prior chemotherapies (≥1 in the metastatic setting) were randomized 1:1 to receive SG or treatment of physician's choice (TPC) until unacceptable toxicity/progression. The primary endpoint was progression-free survival (PFS) per RECIST 1.1 by central review in patients without brain metastases. Patients with brain metastases were allowed if metastases were stable ≥4 weeks. In the intention-to-treat (ITT) population, 19% of patients were age ≥65 years; 12% were Black, and 12% had brain metastases. SG improved PFS and overall survival (OS), respectively, vs TPC in patients age ≥65 years (7.1 vs 2.4 months and 14.7 vs 8.9 months), or of Black race (5.4 vs 2.2 months and 13.8 vs 8.5 months), consistent with outcomes in the ITT population. Patients with brain metastases had numerically higher median PFS with SG vs TPC, but median OS was similar between treatment groups. SG was well tolerated and had a manageable safety profile consistent with the full safety population across all subgroups; neutropenia and diarrhea were the most common treatment-emergent adverse events. These findings confirm the meaningful clinical benefit of SG vs standard chemotherapy in patient subgroups with high unmet needs. SG should be considered an effective and safe treatment option for patients with mTNBC eligible for second-line or later therapy. ClinicalTrials.gov Number: NCT02574455.
© 2024. The Author(s).
Conflict of interest statement
S.A.H. has contracted research with Ambrx, Amgen, AstraZeneca, Arvinas, Bayer, Daiichi Sankyo, Genentech/Roche, Gilead, GSK, Immunomedics, Lilly, MacroGenics, Novartis, Pfizer, OBI Pharma, Pieris, PUMA, Radius, Sanofi, Seattle Genetics, Dignitana, Zymeworks, and Phoenix Molecular Designs; and stock options with NK Max. A.B. received grants from Genentech, Novartis, Pfizer, Merck, Sanofi, Radius Health, and Immunomedics; grants and personal fees from Biotheranostics; and personal fees from Pfizer, Novartis, Genentech, Merck, Radius Health, Immunomedics, Taiho, Sanofi, Daiichi Sankyo Pharma/AstraZeneca, Puma, Phillips, Eli Lilly, and Foundation Medicine. K.P. received honoraria for consultancy/advisory board functions and speaker fees from AstraZeneca, Eli Lilly, Exact Sciences, Focus Patient, Gilead Sciences, MSD, Novartis, Roche, and Seagen; support for attending meetings and/or travel from AstraZeneca, Novartis, Pfizer, PharmaMar, and Roche; and equipment, materials, drugs, medical writing, gifts or other services from MSD and Gilead Sciences. He has participated on a Data Safety Monitoring Board or Advisory Board of Eli Lilly, Gilead Sciences, MSD, Novartis, Pierre Fabre, Roche, Teva, and Vifor Pharma; is a board member of the Belgian Society of Medical Oncology; and is a member of the ESMO Young Oncologists Committee and the ESMO Resilience Task Force committee. His institution has received research grants from or had contracts with Sanofi and MSD; consulting fees from AstraZeneca, Gilead Sciences, MSD, Novartis, Pfizer, and Roche; and payment or honoraria from AstraZeneca, Eli Lilly, Gilead Sciences, MSD, Mundi Pharma, Novartis, Pfizer, and Roche. K.K. received contracts from Incyte, Novartis, Genentech, Lilly, Pfizer, Calithera, Immunomedics, Acetylon, Seattle Genetics, Amgen, Zeno, and CytomX; consulting fees from Lilly, Pfizer, Novartis, Eisai, AstraZeneca, Genentech, Immunomedics, Merck, Seattle Genetics, Cyclacel, and OncoSec Medical; payment/honoraria from Lilly; and support for attending meetings and/or travel from Lilly, AstraZeneca, and Pfizer. He is a member of steering committees at Immunomedics, AstraZeneca, and Genentech. His other financial/non-financial interests include having a spouse who has employment with Grail, Array, and Pfizer. L.A.C. participated on a Data Safety Monitoring Board or Advisory Board of Sanofi Aventis, Novartis, Genentech/Roche, GSK, AstraZeneca/Daiichi Sankyo, and Aptitude Health. Her other financial or non-financial interests include having a spouse who has served on the board of Falcon Therapeutics and who has had involvement in a neural stem cell therapy patent. H.S.R. received grants from Pfizer, Merck, Novartis, Lilly, Genentech, OBI, Odonate, Daiichi Sankyo, Seattle Genetics, Eisai, MacroGenics, Sermonix, Immunomedics, and AstraZeneca; non-financial support from Daiichi Sankyo, Mylan, Pfizer, Merck, Novartis, AstraZeneca, and MacroGenics; and personal fees from Mylan, Puma, and Samsung. A.B. reports grants from Genentech, Novartis, Pfizer, Merck, Sanofi, Radius Health, and Immunomedics; grants and personal fees from Biotheranostics; and personal fees from Pfizer, Novartis, Genentech, Merck, Radius Health, Immunomedics, Taiho, Sanofi, Daiichi Sankyo Pharma/AstraZeneca, Puma, Phillips, Eli Lilly, and Foundation Medicine. V.D. received honoraria from and consulting/advisory roles with Daiichi Sankyo, Gilead Sciences, MSD, Pierre Fabre Oncologie, Roche/Genentech, Novartis, Lilly, Pfizer, AstraZeneca, Eisai, AbbVie, and Seagen; and participated in speakers’ bureaus and support for travel, accommodation, and expenses from Gilead, Roche, Novartis, Pfizer, Lilly, AstraZeneca, Daiichi Sankyo, and Seagen. S.P. has stock/stock options from Gilead as an employee. R.D. has stock/stock options from Gilead as an employee. Y.Z. has stock/stock options from Gilead as an employee. S.M.T. reports grants and personal fees from Immunomedics/Gilead, AstraZeneca, Eli Lilly, Merck, Nektar, Novartis, Pfizer, Genentech/Roche, Exelixis, Bristol Myers Squibb, Eisai, NanoString, Sanofi, Odonate, and Immunomedics/Gilead; personal fees from Puma, Celldex, Seattle Genetics, Silverback Therapeutics, G1 Therapeutics, AbbVie, Athenex, OncoPep, Kyowa Kirin Pharmaceuticals, Daiichi Sankyo, CytomX, Samsung Bioepis Inc., Certara, Mersana Therapeutics; and grants from Cyclacel.
Figures