

FLAMES overlaying anti-N-methyl-D-aspartate receptor encephalitis: a case report and literature review
- PMID: 38664672
- PMCID: PMC11044310
- DOI: 10.1186/s12883-024-03617-z
FLAMES overlaying anti-N-methyl-D-aspartate receptor encephalitis: a case report and literature review
Abstract
Background: In recent years, simultaneous or sequential occurrence of MOG antibody disease and anti-NMDAR encephalitis in the same patient has been reported with increasing frequency. Scholars refer to the overlapping occurrence of these two disorders as MOG antibody disease and anti-NMDAR encephalitis overlap syndrome (MNOS). Cortical T2-weighted fluid-attenuated inversion recovery (FLAIR) -hyperintense lesions in anti-MOG-associated encephalitis with seizures (FLAMES) is a rare clinical phenotype of MOGAD in which cortical FLAIR high-signal lesions are unilateral, with little spread to the cortex and meninges bilaterally. Although cases of FLAMES have been consistently reported. However, to our knowledge, such cases of FLAMES combined with NMDARE are rare.
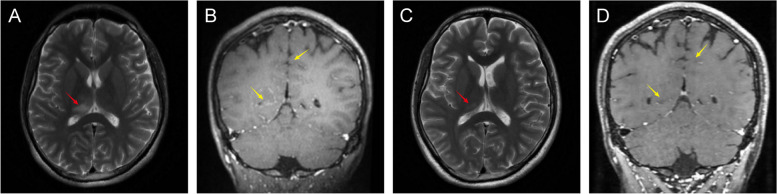
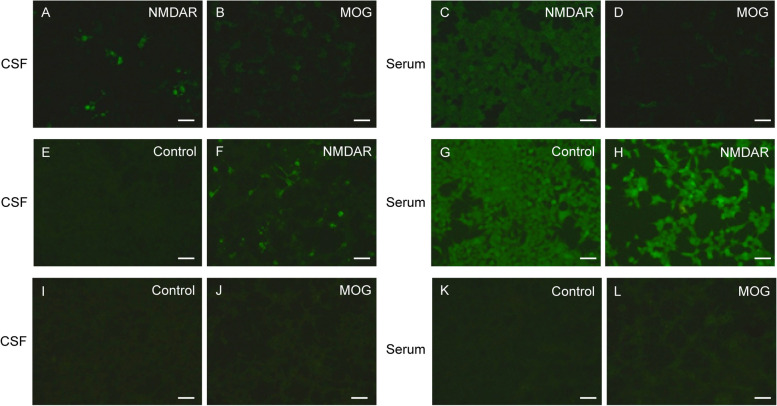
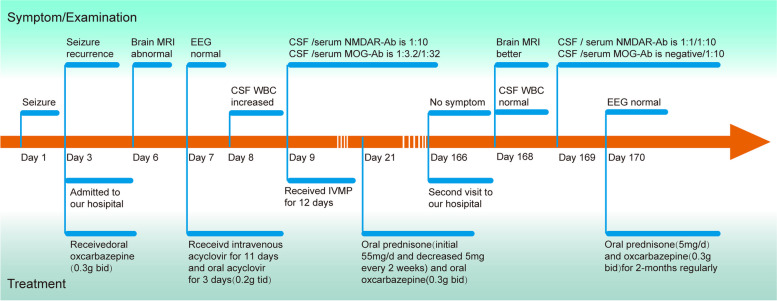
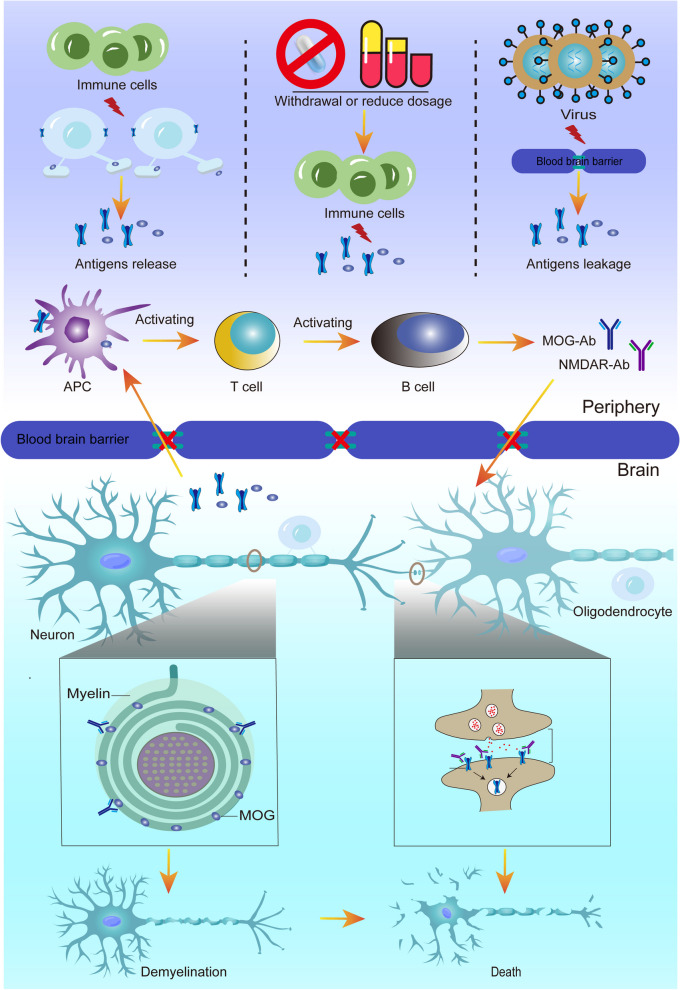
Case presentation: Here, we describe a case of FLAMES combined with anti-NMDARE. The patient was a young male, 29 years old, admitted to our hospital with isolated seizures, whose MRI showed unilateral thalamic and bilateral frontal and parietal leptomeningeal involvement. Since we were unaware of the possibility of bilateral meningo-cortical MOGAD manifestations, the case was initially diagnosed as viral encephalitis and was given antiviral therapy. The diagnosis was not clarified until anti-NMDAR-IgG and MOG-IgG positivity was detected in the cerebrospinal fluid and serum. The patient was then treated with high-dose corticosteroids and his symptoms responded well to the steroids. Therefore, this case expands the clinical spectrum of MNOS overlap syndrome. In addition, we describe the clinical features of MNOS by summarizing the existing literature and exploring the possible mechanisms of its immune response.
Conclusions: Our case serves as a reminder to clinicians that when patients present with atypical clinical manifestations such as seizures, consideration should be given to MNOS and conduct testing for various relevant autoantibodies (including MOG abs) and viruses in both serum and cerebrospinal fluid, as it is easy to misdiagnose the disease as other CNS diseases, such as viral meningoencephalitis. This syndrome exhibits a high responsiveness to steroids, highlighting the critical importance of recognizing the clinical and neuroimaging features of this overlap syndrome for prompt diagnosis and treatment. Furthermore, it enriches the disease spectrum of MNOS.
Keywords: Anti-N-methyl-D-aspartate receptor; Autoimmune encephalitis; FLAMES; Seizures.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Clinical characteristics of children with anti-N-methyl-D-aspartate receptor encephalitis with and without anti-myelin oligodendrocyte glycoprotein antibody.Eur J Pediatr. 2025 Mar 14;184(4):249. doi: 10.1007/s00431-025-06078-9. Eur J Pediatr. 2025. PMID: 40082268
-
FLAIR-hyperintense lesions in anti-MOG-associated encephalitis with seizures overlaying anti-N-methyl-D-aspartate receptor encephalitis: a case report and literature review.Front Immunol. 2023 Apr 17;14:1149987. doi: 10.3389/fimmu.2023.1149987. eCollection 2023. Front Immunol. 2023. PMID: 37138864 Free PMC article.
-
FLAIR-hyperintense lesions in anti-MOG-associated encephalitis with seizures overlaying anti-N-methyl-D-aspartate receptor encephalitis: A case report.Medicine (Baltimore). 2023 Nov 10;102(45):e35948. doi: 10.1097/MD.0000000000035948. Medicine (Baltimore). 2023. PMID: 37960781 Free PMC article.
-
Relapsing MOG-IgG-associated diseases coexisting with anti-NMDAR encephalitis: a case report and literature review.J Integr Neurosci. 2022 Apr 11;21(3):82. doi: 10.31083/j.jin2103082. J Integr Neurosci. 2022. PMID: 35633163 Review.
-
Clinical analysis of a patient simultaneously positive for antibodies of myelin oligodendrocyte glycoprotein and anti-N-methyl-D-aspartate receptor: A case report.Medicine (Baltimore). 2021 Jan 8;100(1):e24234. doi: 10.1097/MD.0000000000024234. Medicine (Baltimore). 2021. PMID: 33429822 Free PMC article.
Cited by
-
Mogad may not only Mimic Immune or Infectious Encephalitis, but can also be Triggered by Viral Infections.Eur J Case Rep Intern Med. 2024 Aug 19;11(9):004764. doi: 10.12890/2024_004764. eCollection 2024. Eur J Case Rep Intern Med. 2024. PMID: 39247246 Free PMC article. No abstract available.
-
Anti-N-methyl-ᴅ-aspartate receptor encephalitis preceding stroke: report of an unusual case with literature review.Encephalitis. 2025 Jul;5(3):71-76. doi: 10.47936/encephalitis.2025.00017. Epub 2025 Jul 10. Encephalitis. 2025. PMID: 40635309 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
